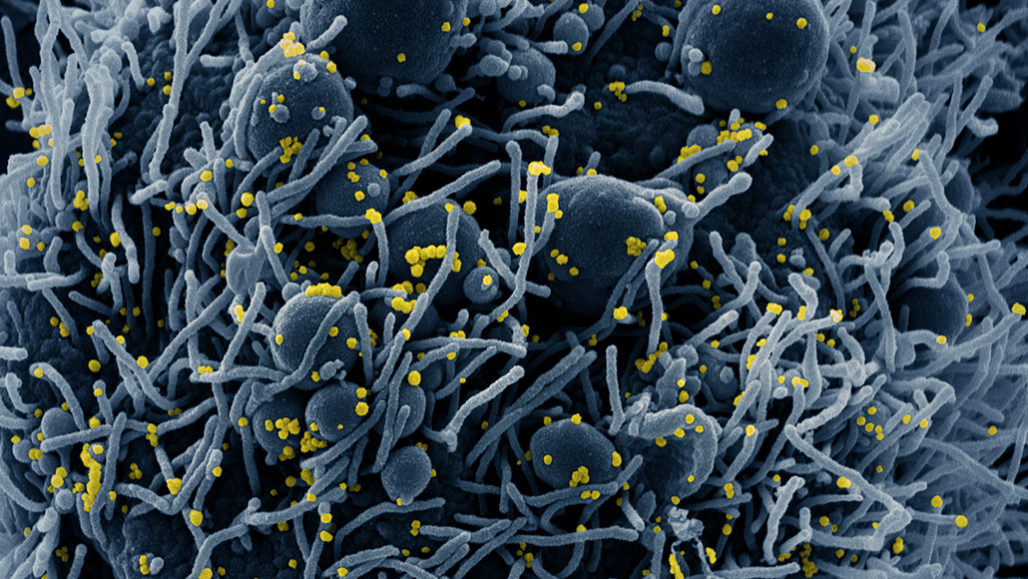
SARS-COV-2 electron micrograph from NIAID– CC license
We know from previous research reported on here that tests of populations without symptoms have shown 20% or more are shedding virus at the time of testing. We don’t know how long they will continue to shed, whether they will develop symptoms later, or what percentage of false negative tests are in these samples. We also don’t know if asymptomatic shedders will develop protective antibodies with time, although that seems reasonable.
With that in mind, we could look at the total population of the United States and say, “how many are now infected?”– although we know the infection rate varies with location, age, and many other factors. Some areas have many infections and rapid spread: mostly large cities. Other areas have few infections but also have rapid spread: mostly rural areas and small towns. A few areas have almost no infections and very slow spread: isolated places.
Just by adding up those two numbers– the percentage of positives in screening studies (ones that sample everyone in a group) and the number of people in the US– we get, veryveryvery roughly, 60 million people. That result is absurd. How could so many people be infected only three months after the introduction of this virus to the US?
The famous author of the web site fivethirtyeight, Nate Silver, introduced an Excel spreadsheet on April 4 that models the spread of SARS-COV-2. The post is titled “Coronavirus case counts are meaningless– unless you know something about testing. And even then it gets complicated.” He links to the spreadsheet at the very end of the post because there is a great deal you need to know before you start playing with the model– and when you look at the spreadsheet, you tend to forget about everything else and possibly ignore the warnings in his post. So read the post carefully, then come back here.
Once I had the spreadsheet in my hot little hands (with the help of an introductory offer from Microsoft for Excel itself), I was entranced. I raised the number of people in the model from 10 million to 330 million and started tweaking the R (the actual number of people to whom each infected person passes the virus). I changed the initial number of people introducing the infection from one to five. I found that, with an R of 3 (well within the range of actual estimates) that dwindled starting on March 1 gradually to 0.4 (consistent with the time that the country went on lockdown), the numbers of actually infected people were staggering. By the end of March, there would be over 110 million people infected.
With an R of 2.7 (the conservative R that the model was shipped with), there would have been 36 million infected by the end of March and 40 million by today. Thereafter, with a lockdown in effect and an R of 0.4, the pandemic would die out. The same is true of most models with a lockdown date of March 1; by now, the infection would be dwindling and very few more people would become infected.
Under these models, with a maximum testing rate of 2 million a day, there would have been about 1.5 million cases detected by today. Unfortunately, there were only 100,000 to 150,000 tests run a day this last week. There have been numerous bottlenecks in raising the test rate, including shortages of swabs and reagents, but in general there has been a lack of federal will and direction to ramp up testing. Despite the population’s worries and the nearly nationwide lockdown, shortages of tests and personal protective equipment (PPE) have continued to hamper our reaction to this pandemic. At the federal level the response is obtuse, opaque, and corrupt.
Based on this simple model, which is available to everyone to tweak and study as they wish, there are possibly on the order of 50 to 80 million people in the US who have had or are having an infection with the novel coronavirus. This guess is really staggering, but it’s based on some simple calculations from real-world numbers.
There is another real-world number that may be consistent with these estimates: yesterday over 1200 people died with COVID-19, not counting the deaths that New York added that had been missed before. Deaths with this virus tend to lag actual infections by two weeks: those who fall ill often seem to be getting along all right until the second week, when they gradually or suddenly start to go downhill and die.
Many of these late deaths may be related to an immune reaction to the virus that surges out of control, attacking the body as well as the virus. Lung, kidney, muscle, brain, and heart tissues seem to be breaking down as the infection progresses. There are also a few who die very quickly very early in the disease process. Some of these people were found at home dead and not counted before.
There is no estimate in the spreadsheet for deaths related to the virus, but this could be easily added. The death rate in the US appears to be roughly 4-5% of those infected. However, accounting for inapparent infections, the death rate may be as low as 0.4%.
My conclusions are that no-one knows how many people in the US have the virus. No-one will know for a long time. By then, we will be left with a wrecked economy and a much larger number of poor people. We will be mourning for many famous people. In November, we will find out whether this nightmare will get worse or will get better. You know what to do– “vote the bums out”.

hospital by Silas Camargo Silao via pixabay.com
Here’s a link to the article. It states that 44% of cases may be transmitted before symptoms appear; this was found in a series in which one patient was definitely known to be infected by another. The study quoted was performed in China in the first two weeks of February. Here’s a quote from the article:
Analyzing 77 infector-infectee pairs allowed researchers to calculate when people are most contagious. The team estimates that contagiousness starts 2.3 days before symptoms begin and peaks 0.7 days before symptoms start.
Based on the information from the aircraft carrier docked in Guam, 60% of cases may be free of symptoms; even when there are symptoms, the patient will be spreading the infection before the symptoms even start. This is the most insidious known virus, clearly highly evolved to spread through-out the human population.

aircraft carrier by David Mark courtesy of pixabay.com
Reuters published a report about the aircraft carrier Theodore Roosevelt stranded in port on Guam on April 16. The Navy has nearly completed testing of all 4,800 sailors on board– 94%– and says that 60% of positive tests (for virus RNA in secretions) were in people who reported no symptoms of COVID-19. This high rate of asymptomatic “carriers” of the virus indicates that previous reports of 25%-50% were underestimates, at least in this relatively young and healthy population.
We need to have nearly universal testing to determine how many people in the US have (or have had) the new virus. This will include antibody testing to find people who have carried the virus and are now recovered. Without such testing, we will not be able to reassure the public that it is safe to come out of hiding.
With about 3.1 million tests performed as of Tuesday and 145,000 tests a day, we are far from this goal. Shortages of testing materials continue, and commercial labs have been unable to perform as many tests as they have capacity. We are not out of the woods yet; in fact, we’re in the rough, so to speak.
There are many conspiracy theories about COVID-19 (coronavirus disease 2019) and the virus that causes it, SARS-COV-2 (severe acute respiratory syndrome coronavirus 2). The sequence of the virus that erupted in Wuhan, China with the first known case November 17, 2019 was published by Chinese researchers in early January (5 genomes were sequenced by January 12). Since then, a large number of sequences (3,965 in the latest report on March 27, with hundreds more every day) have been published for viruses recovered in other locations (particularly the US and Europe, but smaller recoveries in southeast Asia and Australia). The numerous sequences are very closely related, but differences indicate that one variety spread from China eastwards to the western US (with an introduction into Washington State), and another spread west to Europe (with a separate introduction into Washington State, making two clusters in that state; and a second introduction into New York City).
Unlike many other viruses (such as influenza), the novel coronavirus has a correction mechanism that reduces natural variability. It does this by fixing errors in the RNA chain (ribonucleic acid, of which there are 29,903 bases in this virus, each base being one of four types that make up an alphabet) that are introduced by a naturally sloppy duplication system unique to viruses. This is good news for the prospect of a vaccine, because it makes the virus less of a moving target. In comparison, the influenza virus has no correction mechanism and has eight or ten separate RNA chains that can recombine, or mix, with each other. This makes it possible for influenza virus to vary so much that a yearly new vaccine is required to establish immunity.
The virus is closely related to a bat virus– but there is at least 92% whole-genome identity with a pangolin virus. Researchers have found that bats naturally harbor many different viruses, including coronaviruses, without apparently getting sick. A laboratory in Wuhan has been studying the natural reservoirs in bats since the original SARS-COV-1 outbreak in 2002-4. This fact has led some conspiracy theorists to blame the Wuhan lab for the outbreak– either by synthesizing a new genome or by accidentally releasing the new virus and introducing it into a Wuhan “wet market” (a place where many different varieties of live animals are held and custom-slaughtered individually for human consumption). Both theories are at least theoretically possible but extremely unlikely for several reasons.
The first reason is that the Chinese government conducts research into these viruses for prevention rather than as a mechanism for bio-terrorism. To claim that the virus was intentionally introduced would imply that the Chinese intended to slaughter their own citizens first and destroy their own economy, an idea which is akin to national suicide. The Chinese could not have anticipated that the US would fail to protect their own citizens by effectively quarantining international travelers– this fact has resulted in US citizens (China’s richest customer base) being the most affected by a worldwide pandemic of unprecedented proportions.
The second reason is that an accident at the Wuhan laboratory that resulted in the release of the virus would have spread differently. This idea is more tenable but still unlikely. It would have involved a single person who then went on to a wet market (hardly a popular place for a person interested in science and not traditional varietal animal consumption) and gave the virus to a bat, which then gave it to one or two other people, who spread it around. Why would “a Chinese intern” (as the theory goes) have gotten infected, then headed to a wet market instead of going home and giving it to her close relatives?
The third reason is that the coronavirus is not a particularly effective killer, although it is a supremely effective spreader. To be a good bio-terror weapon, a virus needs to be a good, rapid killer that doesn’t spread easily. If it doesn’t kill quickly, it won’t be much use on the battlefield. If it spreads easily, it will infect your own troops as well as the enemy. A virus that leaves over half of the enemy unaffected, while only killing less than four percent of them, doesn’t sound like a very good weapon.
The final reason that this variety of conspiracy theory surrounding the virus is unlikely is the sort of people who are spreading the theory around. They seem to have xenophobia (fear of outsiders) as a political motive for engaging in this sort of thinking. The motives of people who spread conspiracy theories are, at base, highly paranoid and suspicious. They naturally believe this sort of thing because it fits into their world-view (Weltanschauung, in German, or “world-onlook”) which is that “the whole world is out to get me, in particular, because they all hate me, in particular”. People with this Weltanschauung are also highly narcissistic: they believe that the whole world revolves around them, and everything that happens is directed at them by a unified outside force which either seeks to build them up or destroy them.
Narcissism of this type is particularly unrealistic. The whole world in general doesn’t even know that you in particular exist, and that tiny minority who does know of you is hardly unified in their appreciation of your special gifts or hatred and jealousy of your unique qualities. You aren’t unique, and you don’t have special gifts (or do you?). Certain people, world-famous people, are especially prone to this type of thinking because a much larger proportion of the world does know who they are. But, to [redacted]’s eternal chagrin and disappointment, Barack Obama (a person who is much less concerned about how he appears to others, and who is much less attention-seeking) has twice as many followers on Twitter. What’s worse, former President Obama really cares about people in general and has a highly developed ethical sense (qualities that [redacted] completely lacks).
So I am skeptical of this particular variety of conspiracy theory. It may turn out that this virus was accidentally released from a virological laboratory in Wuhan, China– but that doesn’t make any difference to the millions of people who have already been infected. It’s still a naturally derived virus according to the expert virologists, and it’s still a newly evolved “zombie” that takes over your body– for a while, perhaps forever. You can’t run away from it, no matter where it came from. The only thing you can do is stand and fight.

Coronavirus by Engin Akyurt via pixabay.com (open access)
The largest study to date reporting on the use of hydroxychloroquine (HCQ) for COVID-19 involved 181 patients, 84 receiving HCQ and 97 not. The study included all patients hospitalized between March 17 and 31 at four tertiary care centers in France who required oxygen supplementation. Treatment began within 48 hours of admission. Patients were excluded if they had renal failure or another contraindication to HCQ, if they were already on another investigative antiviral drug, or if they already had acute respiratory distress syndrome (ARDS). There were some other criteria of lesser importance; the interested reader is referred to the full text of the article for further information.
The results would be disappointing to [redacted]. About a quarter of the patients in both groups developed ARDS within 7 days; 20.2% of the patients in the HCQ group and 22.1% in the no-HCQ group died or went to the ICU (a non-significant difference). Eight patients receiving HCQ had changes in their electrocardiograms (ECG’s, showing their heart’s electrical rhythms) that required stopping HCQ.
This is the largest reported study of HCQ in COVID-19 to date and it has the strength of a fairly well-matched control group from the same center. It didn’t show any difference in results with treatment, and almost 10% of patients treated with HCQ were stopped due to side effects of irregular heart beats.

photo by Thanasis Papazacharias courtesy of pixabay.com
Multiple news outlets have announced that [redacted] will include “President [redacted]” on the memo line of the stimulus checks to be mailed out to eligible Americans as part of Congress’s virus relief package. His initial attempts to “sign” the checks were stymied by a law that requires a career Treasury employee to sign the checks; this is why paper money has the signature of an unknown Treasury worker on each bill. The law was passed to prevent political advertising from being a part of the money that the Treasury hands out for such things as Social Security, tax refunds, and the like. So He had them include his name on the memo line. This took a change in the programming of the check printers.
The Treasury Department denies that this change will delay the issuance of paper checks, but some IRS employees apparently have said the opposite. Clearly there will be some delay because the inclusion of His name is a change from established procedure. The power that He exerts over the Treasury and other executive branch departments makes this change a foregone conclusion. Whether anyone will be fooled by this into voting for Him (when they otherwise would not) is entirely open to question.
Why are we not surprised? That [redacted] would make the most of any opportunity to advertise his “largesse” (with the taxpayer’s money, eventually, although it is pure debt initially)… when he has falsely claimed to be a multi-billionaire (if he has a net worth, it’s all tied up in unsalable real estate) , a successful businessman (he opened two casinos in Atlantic City a block apart and ran them both into the ground– who loses money from owning a casino?), a straight-talker (with over 18,000 lies and misrepresentations under his belt as President), a representative of the common man (who makes little effort to disguise his disdain for people who are not multi-millionaires, calling them “losers”), and all-around “greater President than Lincoln” (I won’t dignify this claim by bothering to refute it).
Fortunately, I will not be exposed to this naked political propaganda as I am on the “direct deposit” list as a recipient of Social Security retirement checks from the Treasury. I am not holding my breath waiting to receive this money. If He could find any way to punish his opponents by cancelling their payments or with-holding their Social Security, He would do so.
For the reason that I oppose him, and don’t wish to be found out by His internet spies, I have been hiding His name by using [redacted] whenever referring to His August Narcissism. Also, I got tired of waiting for “Don the Con” to catch on; it seemed like the perfect nickname, but no-one refers to Him that way. Finally, I am so sick and tired of seeing him, hearing his voice, or even seeing his name mentioned, that I am sparing myself the nausea that almost overcomes me every time his name is mentioned.
I am heading this post with a picture of Roman coins because the face on the obverse of each is an ancient form of political advertising. The face, for so many illiterate ancients, served as shorthand for the name of the Emperor. The identification of the coin with the ruler served the purpose of telling people where the money originally came from– the Emperor’s personal treasury, in many cases.

death tombstone by Stefan Keller courtesy of pixabay.com
ProPublica reported on April 14 a dramatic increase in deaths at home, especially in cities like Detroit and New York and more so in low-income areas. Detroit has seen a four-fold increase in home deaths and New York has had six times as many as compared to a year ago. At the same time, overall mortality (death) rates have increased. Some people may be dying at home from other diseases, afraid to contact medical help because of the risk of contracting COVID-19 from interactions with the health system. Others are dying with the virus because they were told to shelter in place or because their disease overtook them before they had an opportunity to seek help.
Overall increases in death rates suggest that it is the latter: people are dying from the virus because they didn’t seek help or were told not to come in. The death rate statistics lag behind the rapidly enlarging case counts for two reasons: one, it usually (but not always) takes up to two weeks to die after falling ill, and two, statistics are collected more slowly for deaths, particularly at home.
New York City, among the first to report “data on at-home deaths”, reported last week that about 200 people a day are dying at home or elsewhere outside of a hospital. This compares to an average of 35 a day over the last four years. Middlesex, Massachusetts (of which Cambridge is the best-known city) “reported 317 at-home deaths in March”, a 20% increase over the three-year average. In late February, a conference in neighboring Boston was held that was afterwards linked to more than 100 infections.
This information feeds into a general impression that death statistics for the new virus are an undercount. Many dead people are never tested for SARS-COV-2 because of lack of materials, despite the need to protect autopsy personnel, funeral home workers, and first responders from exposure to corpses that probably are teeming with secreted virus.
The deaths reflect the fact that people 65 and older are at high risk of dying from the new virus. For Massachusetts in March, elder deaths increased by 3.6%, translating to an additional 250 deaths for the state. This leaves out the first two weeks in April, a period during which cases skyrocketed in Massachusetts. The additional deaths make clear that the count of 89 deaths from the virus in the state in March is surely a gross undercount. “As of Monday, Massachusetts’ official COVID-related death count [for April] was more than 840.”
In Detroit, there were 150 “dead person observed” reports “in the first ten days in April”. The average over the last 3 years was 40. Almost all such incidents this year were in areas of low median income, places especially targeted by the virus. In other areas, 911 calls have dropped; in Seattle, “EMT… calls dropped by more than 25% in the first ten days of April compared … [to] … last year.” We don’t know whether emergency calls decreased because people were afraid of contact with other patients or providers with the virus.
The CDC says that death certificates can show “probable” or “presumed” COVID-19 on death certificates if the symptoms prior to death are compatible, even if the patient wasn’t tested for the virus. However, official death tolls mainly “haven’t included people who died before they were confirmed positive.”
Complete death counts will take weeks to compile because of staff shortages and/or aged computers; for California, detailed figures on deaths for the whole state will take a month to obtain and ProPublica will pay $325 for the report. In Hawaii, public health record “processing” has been stopped temporarily.
These at-home deaths show that the numbers we see on TV, even from the Johns Hopkins web site (which is the best), are only “the tip of the iceberg”. We should be very concerned, and we should redouble our efforts to find out why certain people get terribly sick from this virus. The best way to reduce the effects of the pandemic is to find out ahead of time who is going to go into critical condition after infection with SARS-COV-2. Then we can isolate those most at risk and start releasing the rest from their self-imposed “social distancing” and stay-at-home orders.
hospital by Silas Camargo Silao via pixabay.com
Politico’s article from April 14 explains why rural hospitals are “on the ropes”: they were struggling before, and now the community-owned ones can’t get stimulus loans due to an oversight in the $2 trillion bailout package recently approved federally. Read the article for details on which hospitals are closing and which few have gotten loans.
Without properly focused action by the federal government, the medical system is going to be forced through the wringer. Many rural people will be left behind, forced to drove long distances to get medical care. This is an unnecessary disaster, and it is facilitated by the lack of federal oversight and help for rural communities.
Having worked in rural hospitals, I know how important they are to these communities. They are a lifeline for critically injured patients and those who need medical help who can’t drive to the next big city. Without them, these communities will face further contraction and poverty.
Coronavirus by Engin Akyurt via pixabay.com (open access)
Politico reported on April 14 that lab testing for the novel coronavirus has dropped in the last week, as follows:
American Clinical Laboratory Association reported that the number of samples commercial labs handle each day fell from 108,000 on April 5 to 75,000 by April 12. The group’s members, including commercial giants Quest and LabCorp, analyze about two-thirds of all coronavirus tests in the U.S.
Reasons for the drop in testing are complex. One is the testing criteria by the CDC, which prioritize sick people in hospital and healthcare workers who are ill. The criteria have not been changed recently, but they de-emphasize less seriously ill outpatients. Many hospitals are full and emergency rooms overflowing, while others have closed down due to employee illness or budget shortfalls. There are three levels of priority, first seriously ill inpatients and healthcare workers, second people in long term care facilities with symptoms and those over 65 or with chronic conditions with symptoms and ill first responders, and third people in critical infrastructure work with symptoms, and so on. Those who just want to be tested without symptoms are not considered a priority, that is they can’t get tests. You can see CDC’s criteria here.
Public health labs, which do a smaller proportion of tests, said that they have not noticed a drop in test requests, but they do not keep figures on this subject.
Another problem for testing is spot shortages of test swabs and other parts of the test kit. Protective equipment for those who perform tests are also in short supply.
Wyoming’s health labs reported reducing the number of tests because of a shortage of reagents used to do the actual test in the lab.
This drop in testing comes as the case numbers have exploded. I won’t give the latest figures but you can go to Johns Hopkins for the numbers.
Meanwhile, a preprint study on MedRxiv from April 11 showed that self-collected samples performed as well as samples obtained by clinicians swabbing the nasopharynx in detecting active virus shedding. Self-collected testing could reduce a number of problems with using personal protective equipment while obtaining specimens and increase sample collection. Oral saliva and sputum collection could save on swabs as well.
This morning, I saw on TV a report sourced from the New York Post (a rag I don’t read because of its pro-[redacted] bias) that New Jersey has opened a new parking lot test site that uses saliva samples collected by patients, presumably in their cars. Here’s hoping that this newer form of testing will be widely adopted. It is better for two reasons: first, no swabs are needed, and second, interactions with health-care providers are greatly reduced.
I don’t need to tell you that this means trouble for the hopes to “re-open America”. There has been a slight drop in the last week in the rate of new cases, and the rate of testing may be to blame. We can’t deal with this pandemic if we don’t get numbers on how many people have been infected.

a photo of me, by me, looking quizzical. I’m not mad, really I’m not. Or we’re all mad here.
NBC News opinion published a piece today that manifests my opinion exactly. I’ve been thinking this for many years and saying it for the past ten. It’s about time that a national news organization exposed the pernicious conspiracy that is causing “deaths of despair” among working-class Americans. Here’s a link to the opinion piece.
I’m putting my face on this post, because I have little to lose. I’ve given up my place as a little man in the medical hierarchy. I am sick of being compromised. My father was almost a member of this white working class group that almost died from the effects of overly expensive health care. He dragged himself out of poverty, then was struck down by polio. He stumbled, almost literally, and rose again through his own efforts. He had to “use whatever means available” regardless of their effects on his soul and his righteousness. I learned from him, but I only got so far.
I swore that I would never bend to these corporate conspirators who used the free enterprise system to lift themselves above other human beings and then used their advantages to walk all over the people they subjugated. I’m mad now. I was forced to knuckle under to those same corporate leaders in order to make a living. I would have been better off if I had become a mathematician and retreated into the world of numbers.
This pandemic has exposed the bitter reality for many Americans: they cannot access medical treatment for acute illnesses if they do not have insurance. They cannot access health care (preventive medicine) without “health insurance”. Even patients with Medicare are stunned by huge copays for new drugs that are advertised glowingly on television shows that they now watch obsessively. Life is hard, then you die– if you’re an American, you pay a fine of roughly $8,000 a year for using our medical system.
This is wrong. Advanced societies have figured out how to provide medical and health care to their citizens and residents without having to pay a huge premium to the owners of the system. The reason our society (America) pays so much for health is that the people who run the system have an unregulated profit-making system that they have gamed. Lobbyists for these system-runners (pharmaceutical, hospital, doctor, nursing home, and so on) control the levers of power in Washington and all the state legislatures.
Enough. Go and vote the bums out, but be warned: the new boss is just the old boss with a new name. To quote Louis Carroll: “We’re all mad here.”
