Why Don’t Americans wear masks? Because they are narcissistic and psychopathic and just mean.

I was shocked, yes shocked, to learn that Americans are considered more narcissistic than people of other countries. That is the conclusion of actual, peer-reviewed psychological research.
That is why we won’t wear masks. Because we’re narcissists. Thus sayeth the Washington Post.
I can’t think of anything to say that would contradict that assessment. Americans are more narcissistic than people of other countries. Not all of us are, but a lot. A lot of us are rude, aggressive, short-tempered, and just plain mean. A lot of us are even psychopathic sociopathic. We would deny it, but it’s true.
I’m going to do something highly narcissistic. I’m going to leave this post short and sweet. I have some ‘personal’ things to worry about– my wife is sick, and she needs my help. You’ll have to do without my wonderful posts for a day or two.

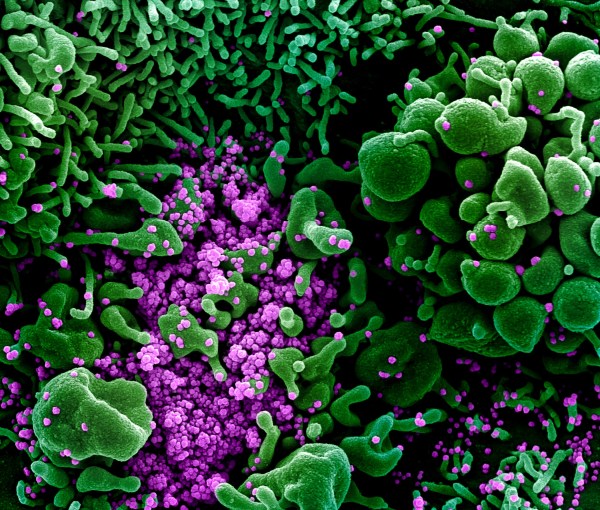
A new article online, published September 21, 2020, on the preprint version of Science Translational Medicine, a subset of Science magazine, looks at the responses of children to SARS-COV-2 infection (COVID-19) and finds a difference in the serum concentrations of immune proteins.
Innate vs Acquired Immune Systems
First, a few words (oversimplified, a summary derived from Wikipedia) about the two main forms of immunity found in all vertebrates (higher animals, with spines): innate and acquired. The innate immune system is inherited from lower forms of life and includes basic responses to all pathogens (organisms which infect other organisms.) The acquired immune system evolved in higher animals and is primarily limited to vertebrates.
The innate immune system starts with a physical barrier (the skin and, inside, the endothelial cells lining the respiratory and digestive tracts.) It continues with specialized immune cells (often called white blood cells or leukocytes) that reside in every tissue of the body. Each individual cell also has innate immune components that include proteins called “toll-like receptors” or TLR. (See also a previous post in which I described a deficiency of TLR-7 which caused severe disease in twin brothers with COVID-19.) Each cell produces “cytokines” (cell-signaling proteins) when it is attacked.
The adaptive immune system is activated by the innate immune system and takes longer to respond. Its components include antibodies and higher forms of immune cells. Immune cells in the innate system (including “dendritic cells” present in all body tissues) break up pathogens and present parts of them (known as “antigens”) to cells in the adaptive immune system.
The acquired immune system develops a memory that enhances the body’s later response to a pathogen after it is defeated the first time. The memory includes antibodies, specialized proteins that are created for each individual type of pathogen in the days and weeks after an infection. Cells that produce antibodies are called “T lymphocytes.” The memory also persists in cells that give us “cell-mediated immunity” and are called “B lymphocytes.” Both types of lymphocytes can persist for decades after a single infection.
The acquired immune system kicks in when the innate immune system doesn’t immediately wipe out an invading pathogen. The acquired system takes four to seven days to rev up in humans.
New Findings About Children
From the abstract of the Science article:
We compared cytokine, humoral, and cellular immune responses in pediatric (children and youth, age < 24 years) (n=65) and adult (n=60) patients with COVID-19 at a metropolitan hospital system in New York City. The pediatric patients had a shorter length of stay, decreased requirement for mechanical ventilation and lower mortality compared to adults. The serum concentrations of IL-17A and IFN-γ, but not TNF-α or IL-6, were inversely related to age. Adults mounted a more robust T cell response to the viral spike protein compared to pediatric patients as evidenced by increased expression of CD25+ on CD4+ T cells and the frequency of IFN-γ+CD4+ T cells. Moreover, serum neutralizing antibody titers and antibody-dependent cellular phagocytosis were higher in adults compared to pediatric COVID-19 patients. The neutralizing antibody titer correlated positively with age and negatively with IL-17A and IFN-γ serum concentrations.
https://stm.sciencemag.org/content/early/2020/09/21/scitranslmed.abd5487
The higher concentrations of IL-17A and IFN-gamma in children are related to their innate immune systems, which respond to unfamiliar infections. IL-17A is a cell-signaling protein that promotes inflammation by starting a cascade of cell signals resulting in attraction of immune cells to areas of inflammation– areas invaded by pathogens like the novel coronavirus. IFN-gamma is another cell-signaling protein which is important to virus immune responses.
IL-6 (another cell-signaling protein) has a broad range of activity, both pro- and anti-inflammatory, and high levels are associated with severe COVID-19 with a poor prognosis. TNF-alpha (yet another cell-signaling protein, formerly known as cachectin and now called simply TNF) induces fever, cachexia (loss of weight associated with illness) and other signs of inflammation. At extremely high levels, TNF can cause septic shock. Both TNF and IL-6 inhibit viral replication (multiplication of viruses within a cell.)
Conclusions About Children
From the article:
Dual cytokine (IL-17A and IFN-γ)-producing resident memory cells have been described in the lung (19) and a protective role for Th17 cells has been described in pulmonary infections (20). Possibly, the higher concentrations of IFN-γ and IL17A in the serum of pediatric patients with COVID-19 reflected increased expression by cells in the respiratory tract, and these local cytokines may have protected the patients from progressive respiratory disease. …
The age-related difference in IL-17A concentrations in serum is consistent with described dysfunction of innate immune responses in older individuals (22). Decreased expression of pattern recognition receptors such as RIG-I by monocytes has been found with aging and has been postulated to account for reduced Type 1 interferon release. Invariant NKT cells, which secrete IL-17A and have cytolytic function, also decrease in number and function with aging (23). …
The bottom line is that higher levels of IL-17A and IFN-gamma appear to show the stronger innate immune response of children to SARS-COV-2 exposure and are probably related to robust reaction of cells (particularly dendritic cells) in the lung to infection. This stronger immediate immune response, not dependent on the acquired immune system but due to quick reaction by the innate immune system, may explain why children show fewer and milder signs of infection when COVID-19 occurs.
At the same time, delayed occurrence of the MIS-C syndrome probably is due to late over-reaction of the acquired immune system, two or more weeks after infection. This syndrome, while dramatic, usually has a more benign prognosis– that is, children usually recover from it (although not always.)
Lower levels of “serum neutralizing antibody titers and antibody-dependent cellular phagocytosis” in children appear to be due to the fact that the innate immune system has terminated the SARS-COV-2 infection quickly and stopped the acquired immune system from being fully activated.
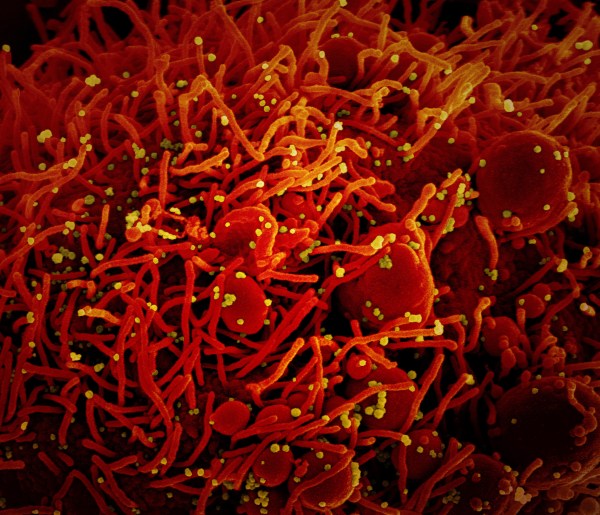
A preprint published on MedRxiv dated September 22, 2020 revealed that a mutation in SARS-COV-2 RNA has taken over in Houston (and probably many other areas) based on sequencing of over 5,000 cases. The mutation causes the replacement of a single amino acid at location 614 in the spike protein. It is known as D614G (arginine –D– replaced by glycine –G.)
This mutation was discovered in February and was followed in the United Kingdom (UK) with sequencing of over 25,000 cases there. A paper discussing this sequence database was published in MedRxiv on September 1, 2020. The findings of that paper agree with the Houston paper in all important respects but the new paper adds more information.
The mutation produces viral particles with many more spikes on their surfaces. It is these spikes that the virus uses to attach to host cells by grabbing on to their angiotensin-converting enzyme 2 (ACE-2) receptors. ACE-2 receptors are present on the outer membranes of most endothelial cells (those that line the inside surfaces of the nose, throat, eye conjunctiva, and gastrointestinal tract as well as inside blood vessels.)
This mutation increases infectiousness but not lethality. Initial viral loads were increased in the nasopharynxes (noses and throats) of patients infected with the mutated virus, but these patients were no more likely to have severe disease. This mutation has taken over, outcompeting the previous version of the virus by spreading more easily.
The fact that infections with this mutation are no more severe is logical when we consider that making the patient sicker doesn’t help the virus spread– killing the patient isn’t good for the virus.
The sequencing of so many separate viruses has revealed numerous mutations, many of which were seen in only a few cases. The authors of the paper advocate for virus sequences from many more patients to help us monitor the spread of the virus and trace contacts.
Another reason to sequence more viruses is that some mutations will reduce the ability of antibodies to neutralize the virus. In fact, the authors found that monoclonal antibody CR30022 was less able to recognize some mutations. This could be a factor in patients who have repeated infections with different strains of the virus.
This may also impair the ability of manufactured monoclonal antibodies to treat the disease in new cases. Monoclonal antibodies are being actively studied as a treatment for COVID-19, but the fact that they have to be separated and manufactured (which takes several months) may make them too late to be helpful in some new cases.
Mutations could also affect the ability of vaccines to provide protection against the virus. If this happens repeatedly, we could find ourselves in the same position as we are with influenza: we will need new immunizations on a yearly basis.

He’s not. He gave up his board certificate in 2005 after creating his own “National Board of Ophthalmology” (see Wikipedia; also see Jennifer Rubin’s column in the Washington Post from seven years ago, titled “Rand Paul has another problem.”)
He’s also lousy as an infectious disease doctor; see his performance with Dr. Anthony Fauci in the Senate: “Fauci finally loses his patience“.
All this we have to thank for that guy in the White House.

A 28 year-old second-year resident at a hospital in Houston fell ill with COVID-19 and was taken to the emergency room (ER) on July 8, 2020. She had been working in the ER as a resident physician and was exposed to acutely ill COVID-19 patients there. Her name was Adeline Fagan, and her story was told in People magazine on September 21.
She did not respond well to being put on a ventilator on August 3, and extracorporeal membrane oxygenation (ECMO) was used instead. She developed a “massive brain bleed” (cerebral hemorrhage) and died the next day. Her death was announced on a GoFundMe page September 19.
According to CNN, she had suffered from asthma, upper respiratory infections, and pneumonia in the past, but was quite well and working full time when she got sick in July. I’m guessing that she had just started her rotation in the ER when she was infected, because resident rotations start on July 1.
The reason I brought up her death is that multiple news agencies have announced that there have been officially 200,000 deaths from COVID-19 as of yesterday (although there were more than that suspected based on overall excess death rates as early as a month ago.)
In addition, Justice Ruth Bader Ginsburg died last Friday. She was 87 years old and had survived colon cancer and two other types of cancer before succumbing to pancreatic cancer. This last type of cancer has an extremely poor prognosis even when it is caught early.
It is likely that the president had advance warning of her death, because he announced a new short list for Supreme Court candidates just a week or two ago. The Senate Majority Leader announced about an hour and a half after her death came out that he would bring up a replacement to a vote as soon as the president nominated somebody.
This was promised by the president shortly after. He is only waiting until after the funeral to announce someone. There is little or no question but that a replacement Supreme Court Justice will be confirmed within the next 45 days, that is before the presidential election.
This is a sin and an abuse of power. This Justice had been sitting for 27 years and had helped to win historic improvements in civil and human rights for previously marginalized citizens. Now the extreme right wing Republicans will have an “opposite” Justice.
There is tragedy and despair everywhere in this country. The only thing that will cheer me up is if a Democratic president is elected by a landslide in November. Then we can proceed with taking back power for the people who have suffered so long under the yoke of the “conservative” power-mad Republicans.
For the last 52 years, ever since Richard Nixon was elected President, we have gone backwards as a country despite the improvements on the margins that were shepherded by Ruth Bader Ginsburg. It is time to return to going forwards as a whole country. The only way to do that is to take power, constitutionally, away from the retrogressive “conservatives.”
There is talk of doing away with the Senatorial filibuster and expanding the Supreme Court to make up for the loss of two Justices to the machinations of the current Senate Majority Leader. Both changes will be perfectly legal and justified if the Democrats win back the Senate.
It will not be easy. A landslide election victory for Joe Biden is in the cards, but the current president is almost certain to contest the results all the way to the Supreme Court. He will be in for an unpleasant surprise even if he has a new Justice in place– there is little that can be done to nullify an obvious landslide. It is quite possible that he will use other, less conventional means to contest the election– such as having states with Republicans in power certify the wrong results.
All of the disasters that have happened, just in the last nine months, not to mention the last four years, will be less than the disaster that will befall us if this election is lost to the Republicans. Please vote, and encourage all your friends who can vote to do the same. It’s probably too late to move to Nevada to vote there, if you haven’t already done so.
N95 masks: failure by federal administration to use DPA leads to persistent shortages: WaPo
The Washington Post published on September 21 an account of why there is still a severe shortage of N95 masks. The article attempts to answer a seemingly simple question: “Why is the world’s richest country still struggling to meet the demand for an item that once cost around $1 a piece?” This piece (and other coronavirus coverage) is available for free on the WaPo website.
For those who are not yet aware of what an N95 mask is, they are simply masks that filter out 95% of airborne particles. This Wikipedia page has a thorough explanation of what these masks do. The medical type of N95 mask is certified by the National Institutes for Occupational Safety and Health (NIOSH) and cleared by the Food and Drug Administration (FDA), and recommended for use against infectious bacteria and viruses. They are made of nonwoven polyester fiber and electrostatically charged to trap small particles.
The Washington Post article explains that the federal administration could have obtained a machine capable of making 1.5 million N95 masks a day that was created with funding from the Department of Health and Human Services (HHS) in 2018– but it failed to purchase the rights despite having paid for its invention. What is worse, in early 2020, an opportunity to ramp up production of the masks offered by a company that was ready to do so was turned down.
As a result of the administration’s dropping the ball, the only American manufacturer of N95 masks is 3M, and it can only make so many. 3M is primarily motivated by profit in making masks– there is no government mandate. They will be producing 160 million a month by December, but that still will not be enough to meet demand. The administration has not invoked the Defense Production Act to order companies to make the masks, which would guarantee companies a fixed profit and a market for all they could make.
All of this information, and much more, is available for free in the article by the Washington Post, which is making all its coronavirus pieces subscription-free during the pandemic. The article includes a clear pictorial explanation of how the masks work. It also has personal-interest bits on people who use the masks. It is well worth taking the time to read for an understanding of why the masks are needed and what the administration has failed to do to help.
As a postscript, there are messages about wearing glasses or goggles as well as a mask that make an argument that they give significant additional protection. Apparently, according to Dr. Anthony Fauci, goggles are a good idea– see this People magazine article or this New York (NYMag) article.
Multiple drug companies are actively researching monoclonal antibodies for treatment of COVID-19. Lilly announced success (see this Medscape article from September 17) in reducing hospitalizations with one of its antibodies in clinical trials. The trials, in 302 patients with mild to moderate symptoms, reduced hospital stays or emergency room visits from 6% (with placebo) to 1.7% (five patients) of the treated group.
Monoclonal antibodies are given in a single dose intravenously, and one shot delivers antibodies that last about a month. The shots could be used either for treatment, early or late during the disease, or prevention. It is not yet known when during infection would be the best time to administer the shot.
Monoclonal antibodies are derived from the serum of patients who are convalescing after acute viral infection. Each individual type of antibody is produced by a single immune cell which can be cloned– thus, monoclonal. The antibody is directed against a specific part of the virus, usually the spike protein with which it attaches to an endothelial cell during infection.
Once the monoclonal antibody is identified (separated from the large group of different antibodies circulating in a recovering patient’s serum) it can be produced by a specific segment of DNA. That DNA segment is transferred into another type of cell which can be cultured in a “broth” that nourishes the cells– in this case, a cell from an animal embryo.
Large numbers of these cells are cloned and grown over several months in a tank. The antibody protein is then purified from the broth, sterilized, and put into cold storage. This process is time, labor, and money-intensive.
Sufficient antibody of one type for about 100,000 treatments has been collected in this way. If the continued trials with this antibody are successful, Lilly will seek approval from the Food and Drug Administration (FDA) to market the antibody for clinical use.
Regeneron Pharmaceuticals and Vir Biotechnology, among others, are also working on additional monoclonal antibodies for use in COVID-19. The treatments are likely to be very expensive because of the complex and lengthy manufacturing process.

According to several news accounts, Alan Dershowitz filed a civil lawsuit on September 15, 2020 against CNN for defamation of character. According to the suit, CNN implied that he had “lost his mind” when it “unfairly abridged” the argument he made during the Senate impeachment trial in January. The suit demands $300 million in compensation.
The argument at the impeachment trial was apparently a lengthy one, difficult to summarize. According to the “Law and Crime” blog by Dan Abrams on September 15:
Dershowitz’s allegations stem from news coverage of his argument about the kind of quid pro quos a sitting president may engage in while office—provided that the exchange is done with the intent of winning re-election in the public interest and not in violation of some law. While his theory was widely panned by attorneys and legal experts across the media, Dershowitz claimed that CNN intentionally omitted portions of his argument to make it appear as though he was arguing “the exact opposite of what he said.”
https://lawandcrime.com/lawsuit/alan-dershowitz-files-300-million-lawsuit-against-cnn-for-portraying-him-as-an-intellectual-who-had-lost-his-mind/
It seems that the president’s “intent” was the crux of Dershowitz’s argument– he was saying that as long as at least part of the president’s intent was not corrupt, then the quid pro quo was not unlawful. That is, the president’s desire to be re-elected was at least partly in the public interest.
So he claims that CNN’s omission of that part of his argument was defamatory. Some of the comments to the blog post point out that under Florida case law, quoting only part of a statement is not defamatory… this is unclear to a non-lawyer, but so is the rest of this case.
Dershowitz’s entire argument was “widely panned”, as in, most media commentators considered it fatuous. A commenter on the blog compared the argument to justifying robbing a bank with the intent of testing the bank’s security systems– in the bank’s customer’s interest– or to eating human flesh to see how it tastes– as a food critic. Personally, I do not see how winning re-election could be in the public interest, especially not for the current sitting president.
The $300 million demanded in this case appears to be completely imaginary. Dershowitz’s suit is likely to be dismissed. He is, as it happens, a public figure, so he is not easily defamed unless “actual malice” can be shown. His support of the current president has made him persona non grata among the liberal elites whose company he used to enjoy.


A new article in the Washington Post dated September 16 reveals that deaths from dementia have dramatically increased since nursing homes were isolated by the COVID-19 pandemic in March. Here’s a quote from the article:
more than 134,200 people have died from Alzheimer’s and other forms of dementia since March. That is 13,200 more U.S. deaths caused by dementia than expected, compared with previous years, according to an analysis of federal data by The Washington Post.
https://www.washingtonpost.com/health/2020/09/16/coronavirus-dementia-alzheimers-deaths/?arc404=true
That is a roughly ten percent increase in death rates, not due to the novel coronavirus, but due to depression, anorexia (loss of appetite), falls, lung infections (like pneumonia), and “sudden frailty.” Many of those who declined and died had been stable for some time.
The declines appear to be due to isolation. Family members are no longer allowed to hug, kiss, or hold hands. Visits, even by video phone, have decreased as well. Patients are no longer allowed to socialize among themselves. Activities like Jazzercise helped patients physically and mentally, but they are no longer possible in isolation. Patients are no longer able to eat together.
These contacts may have maintained some degree of mental stimulation that prevented continued declines. Without them, patients are becoming more depressed and anxious. Reduced physical activity and mental stimulation causes physical deterioration.
Nursing homes have struggled with borderline fiscal support for years. Patients’ relatives have filled in with feeding, bathing, and stimulation to supplement paid work by nurse’s aides. The relatives can no longer perform these assisting activities, which leads to poorer care.
The money that has been provided by Congress for emergency help has not gone to nursing homes. Testing is still minimal, and personal protective equipment is in short supply. Nurse’s aides, who are afraid of being infected, have stopped going to work in some cases and are more difficult to hire.
This is one reason why 40% of the coronavirus deaths in this pandemic have occurred in nursing homes. To add to the increased vulnerability of elderly, chronically ill patients to the virus, there is the fragility of nursing home care. Now it is clear that patients are dying of simple neglect due to quarantines and understaffed homes.
Postscript:
Here’s the most popular comment to the Washington Post story:
The point of a public health lockdown is to buy a short amount of time to allow classic public health measures to be implemented to limit disease spread. Since the administration has not implemented even basic public health measures ( and in fact, has thwarted attempts of the CDC and the states to do so), we are stuck in this state of near-permanent lockdown. It did not have to be this way.
Thanks to you, Mr. Wan, for documenting the devastating impact that this prolonged lockdown has on patients in assisted living and nursing homes.
submitted by Blues89
The rest of the country has been “opened up” in part due to armed demonstrators invading the state’s legislatures– but the nursing homes are still “locked down.” Public health measures like personal protective equipment and frequent testing are simply not available. Nothing has been done to relieve the conditions in nursing homes.
Post-PostScript:
Here’s another popular comment, with some practical advice:
This is a tragic consequence of the inadequacy of public health in the U.S. My mother is 91 and has been in assisted living for almost four years. She was only recently been given a diagnosis of dementia. Her cognitive abilities and her mood have seriously declined since our frequent visits were halted. Luckily, her doctor agreed to write a referral for hospice. The primary benefit— which we didn’t even know about when we asked for hospice — is that we are now allowed to visit her in her room daily, rather than once a week for a half hour on the patio. The rules differ between facilities, but anyone in a similar situation should look into hospice. At least here in NJ, we didn’t need a definitive terminal diagnosis (e.g. “she has six months”) and many people have told me what a blessing it was for them. I urge everyone to look into this wonderful program!
submitted by Liz Pago
