
photo by Susanne Jutzeler courtesy of pixabay.com
The New Yorker on April 20 published an article by Jim Yong Kim titled “It’s not too late to go on offense against the coronavirus”.
The five main categories of offensive action against the novel coronavirus (SARS-COV-2) are as follows: 1) social (physical) distancing; 2) contact tracing; 3) testing; 4) isolation; and 5) treatment.
These strategies have been employed by the countries with the best records against the virus: South Korea, Singapore, Taiwan, and Hong Kong. The article describes how these strategies can bring the spread of the virus under control, even at this late date. The author describes how Massachusetts (to which he is a special advisor) is beginning to implement the elements of this aggressive plan. The Broad Institute is also going to help.
We need considerable help to implement these elements. Contact tracing requires people who can do the “shoe leather” detective work. Isolation requires direct assistance to those who are quarantined, to help them with food, shelter, and medicine– and to explain to their bosses why they can’t come to work. Medically supervised isolation facilities are also needed. Treatment requires research and production of new medicines.
All of these things require a lot of work. It is better to engage in this work than it is to just shelter in place and hope for the best. Rather than just throw money at impacted businesses, we should invest in hiring and supporting the people who can do the work needed to trace and isolate all contacts.
From the article:
When we presented our plan to Governor Baker, he didn’t say that it was too expensive or too hard or too late. He said, “We have to do this. We have no choice. It feels like we’re just sitting and waiting. We have to go on offense against the virus.”

photo courtesy of pixabay.com
Reported by the Washington Post on April 22. The death only came to light now because tissue samples from the autopsy were sent to the Centers for Disease Control (CDC) for analysis by the county medical examiner and analyzed for the new virus. A second patient who died February 17 was similarly analyzed and announced at the same time.
[redacted] and Dr. Deborah Birx also claimed that the US has one of the lowest death rates from the virus in the world– a patently false claim. According to the Post, the US has a higher rate than 101 other countries.

puzzle by Gerd Altmann courtesy of pixabay.com
The Washington Post published a story on April 19 about patients missing from the normal retinue of emergency cases: those with the usual non-infectious illnesses such as appendicitis, heart attacks, strokes, cholecystitis, and gallbladder stones. Mount Sinai cardiovascular surgeon John Puskas was quoted as saying, “Everybody is frightened to come to the ER [emergency room]”. People who don’t come in with early signs of these acute emergency conditions are going to come later, when their symptoms have reached unbearable levels, and are going to be harder to help, with more complications or even death from untreated illness.
One anecdote, a patient with appendicitis in his twenties: he tried to “tough it out” with over-the-counter painkillers, until his appendix had ruptured and formed a large abscess in his belly. He had to have open surgery (where a laparoscopy could successfully have removed an unruptured appendix) and a colostomy, meaning he was forced to spend days in the hospital. He would have to return later to take down the colostomy to restore normal bowel functioning. He had to take antibiotics for an extended period and could have died. He was afraid to come to the hospital early, when his condition could have been quickly treated, because he was afraid of contracting the virus– even though, at his age, he might have had an asymptomatic infection or quickly recovered without any problems.
Evert Eriksson, trauma medical director at the Medical University of South Carolina, described this patient and said, “… 70 percent of the appendicitis on my service right now are late presentations. What happens when you present late with appendicitis is, we can’t operate on you safely.” Yet his 700-bed hospital is only 60 percent full because most of their patients have been discharged to make room for an expected surge of coronavirus patients.
A report accepted April 7 as a pre-print in the Journal of the American College of Cardiology (cited in the Washington Post article) documented a 38% reduction in patients admitted for percutaneous coronary artery revascularizations at nine major cardiac catheterization labs in the Northeast and Midwest in March 2020 as compared to the previous fourteen months. These patients, all with acute myocardial infarctions (heart attacks) with ST segment elevation (a sign of complete blockage of a major coronary artery to the heart), simply were not seen. Some of them would have died without this treatment; the rest suffered severe heart damage and were left with weakened or reduced heart function. This happened at a time of stress when heart attacks would have been expected to increase rather than decrease.
From the Washington Post article:
A Gallup online poll taken March 28 to April 2 asked people with different conditions how concerned they would be about exposure to the coronavirus if they needed “medical treatment right now” at a hospital or doctor’s office. Eighty-six percent of people with heart disease said they would be either “very concerned” or “moderately concerned.” Among people with high blood pressure, the figure was 83 percent.
One major stroke center found a more than 60 percent reduction in referral calls from hospital ERs about possible stroke patients and a more than 50 percent reduction in patient phone calls. It seems that patients with mild or moderate stroke symptoms are simply not calling in for help.
Some conditions are less common because of the almost universal “stay at home” orders blanketing the country. There has been a steep drop in car crashes, for example. There has not been a drop in domestic violence incidents.
Some heart attacks may be prevented by people not going to work and not exerting themselves at home. Others may be prevented by not eating high-fat restaurant meals and the drop in air pollution (and air pollution, especially particulates, does bring on heart attacks). Some patients with heart attacks may never make it to the hospital because emergency medical protocols have changed. Those who suffer cardiac arrest and do not have return of spontaneous heart action (and circulation) after resuscitation efforts are not being taken to the ER, but are declared dead in the field.
Finally, some patients with COVID-19 may have double diagnoses: both new virus disease and heart attacks at the same time. Only time and thorough review of all findings will tell us where all the emergency patients have gone.
Deep uncertainty about the new virus and its effects on patients with pre-existing conditions has made the job of treating all patients during this pandemic much harder. We already know that conditions like diabetes, high blood pressure, and heart disease make infections with the new virus worse. What we don’t know is why other factors, many of which are more prevalent in elderly patients, make recovering from an infection so much harder. We don’t know what other genetic or social conditions are doing to make the infection and death rates so much higher in African-American and Caribbean-American patients; we just know that things are much harder for black people.


klee flower by cocoparisienne courtesy of pixabay.com
Medpage today has an article published April 20 titled “Fear of the False Negative COVID-19 test” which describes concerns over the false negative rate of the virus antigen nasopharyngeal swab test, especially for healthcare providers. The article states that, with a 10% prevalence of truly infected COVID-19 patients, out of a million healthcare providers, 40,000 will show false negative tests. This is a serious problem both for providers and patients, and the first statement in the article underestimates the extent of the problem.
In fact, the rate of positive tests in patients later confirmed to have COVID-19 is only 70-80%. A Chinese study of 51 patients who had abnormal chest CT, only 71% (36/51) had positive RT-PCR nasopharyngeal swabs at the first go. One patient required four swab tests to isolate the virus. From the CT study:
50/51 (98%) patients had evidence of abnormal CT compatible with viral pneumonia at baseline while one patient had a normal CT. Of 50 patients with abnormal CT, 36 (72%) had typical CT manifestations (e.g. peripheral, subpleural ground glass opacities, often in the lower lobes and 14 (28%) had atypical CT manifestations.
From the study’s conclusions:
In our series, the sensitivity of chest CT was greater than that of RT-PCR (98% vs 71%, respectively, p<.001). The reasons for the low efficiency of viral nucleic acid detection may include: 1) immature development of nucleic acid detection technology; 2) variation in detection rate from different manufacturers; 3) low patient viral load; or 4) improper clinical sampling. The reasons for the relatively lower RT-PCR detection rate in our sample compared to a prior report are unknown. Our results support the use of chest CT for screening for COVD-19 for patients with clinical and epidemiologic features compatible with COVID-19 infection particularly when RT-PCR testing is negative.
Compared to rates of positive tests done by bronchoalveolar lavage (fluid taken from deep in the lungs by bronchoscopy, a tube inserted down the throat into the lungs to observe to bronchi), with a positive rate of 93%, the nasopharyngeal swab is inadequate for making a diagnosis. This explains why the Chinese decided to include abnormal chest CT findings as a criterion for diagnosis of COVID-19 cases.
A patient who presents with cough, fever, chest pain, and shortness of breath is likely to have viral bronchitis or pneumonia. If the test done by nasopharyngeal swab is negative, the patient may be falsely concluded to have influenza (or an influenza-like illness caused by another virus or a bacterium). Tests can be performed for the influenza virus, cold coronaviruses, and bacteria, and if these are negative, further suspicion may fall upon the new virus– but this state of affairs will lead to patients not being adequately isolated and not included in case counts.
More seriously, if the patient is a healthcare provider, and they go back to work, they may wind up infecting many patients who would not otherwise be exposed.
The only solution is to presumptively isolate all patients who have symptoms consistent with influenza-like illness. This may perhaps have been the best course of action even if the new virus were not known to exist, since it would lead to patients not being exposed to other contagious illnesses that could have equally adverse effects clinically.
The clinician’s learning curve for this viral pandemic is steep, indeed. We need to take instruction from the Chinese, who, despite their suspicious behavior in regard to case counts (which subject is open for discussion, either way), have provided us with a great deal of information about the disease, making diagnoses, and ways to combat its spread. We (the editorial “We”) cannot condone totalitarian behavior by the Chinese government.
We must seek voluntary agreement to isolation, surveillance, and control because agreement is essential to win this fight. We can only obtain voluntary compliance with strict measures by radical transparency and protection of the identities of those who are affected. This is seen with the South Korean model, where they have gained the upper hand and are continuing the fight with almost complete buy-in of the entire population of South Korea.
We call for all Americans to be given access to “smartphones” that are programmed with infection tracing, news apps, and control measures. This includes notification of all significant developments in news of the campaign and information about confirmed cases that have “crossed the path” of the smartphone owner so they can be fully informed and take precautions to prevent illness or inform disease-control teams if symptoms arise.
We also demand that tests be made available to all Americans, both acute (virus RNA detection by nasopharyngeal swab or sputum analysis) and chronic (serum antibodies or serology) as soon as is possible. If it appears to be necessary, the president must invoke the Defense Production Act to order private industry to develop and market testing supplies and equipment. A small step in the right direction was announced yesterday: an order to produce 20 million swabs for use in the virus detection test kits.
Much greater efforts are needed if we are to rescue the economy and return the US to a leading place among the nations of the earth. I/we call upon all Americans to “vote the bums out” and begin a program of radical restructuring that will work to end the obfuscation, corruption, and incompetence of the current administration led by a sociopathic, narcissistic, nepotistic con-man. We can do no less for our fellows, especially those who have been left behind and are being mowed down by the pernicious new virus. Members of minority groups, including Native Americans, African-Americans, Caribbean-Americans, Asian-Americans, and Latin Americans, have been discriminated against in the past and are now being affected in greater numbers by this virus. I/we call upon all Caucasian-Americans (European and British) to stand together with your fellow Americans of color to defeat the seditious conspiracy of plutocrats who have seized control of this country and have been running it into the ground since their Electoral College victory in 2016.

photo by David Mark courtesy of pixabay.com: mountains of South Korea
The New Yorker published an article dated April 17 about COVID-19 in South Korea. These articles should be available without a subscription since they are related to the novel coronavirus. The contrast between how SARS-COV-2 is treated here and there could not be starker. We test only people who are either very ill or have been in close contact with someone sick. Even then, testing is spotty. There is next to no tracing of the movements of people with positive tests, and no-one wears a mask unless they live in New York City.
In South Korea, they had a bad experience with “Middle Eastern Respiratory Syndrome” (MERS). After the scandal, in which it was discovered that the government had not given out critical information and allowed transmissions of the virus, illnesses, and deaths, they passed a law. Now they test everyone coming into the country, sometimes on multiple occasions. The tests only take 24 hours to finish, and the results are sent to the patient by text message. Those who test positive are quarantined or admitted to the hospital. Their movements are traced and publicized, and everyone who has been in contact with them comes in to be tested. Public places where they have stopped are thoroughly cleaned; people avoid them anyway, even though they pose no risk after being sanitized. Every bit of information is shared widely; reports are sent to all the smartphones in the country. As a result, toilet paper is widely available and there is no hoarding.
Under the terms of South Korea’s Infectious Disease Control and Prevention Act—passed after the 2015 mers outbreak, during which the government’s withholding of critical information contributed to further transmissions and deaths—it is now required to publish information that can include infected people’s travel routes, the public transport they took, and the medical institutions that are treating them.
The South Korean government rations face masks: people are allowed to buy two a week. They are the surgical type so long familiar from movies, not home-made. Only high-risk establishments like night-clubs and churches have been closed; even then, closures are voluntary. Places can stay open if they observe mask-wearing and a two-meter distance between patrons. Most churches have switched to on-line services anyway. Restaurants are still open.
Having a universal health care system is a big help for South Korea. The infection-control law allows for close contact tracing using credit-card information, closed-circuit TV cameras set up in public places, and so on, but it prohibits the use of this information for anything other than infection control.
South Koreans have decided that, during an infectious-disease outbreak, there is a strong, pragmatic case to be made in favor of what might be called virtuous surveillance—a radically transparent version of people-tracking that is subject to public scrutiny and paired with stringent legal safeguards against abuse. Despite its imperfections, South Korea’s policy is striking for the fact that it brings the mechanisms and outcomes of surveillance into the public forum. In doing so, it appeals to a deeper sense of civic trust—the belief that, in a crisis, the citizenry can be relied upon to play its part.
South Korea has some big advantages over the United States. One is universal health “insurance”; another is the sense of community spirit that allows democratic functioning in a time of emergency.

Coronavirus by Engin Akyurt via pixabay.com (open access)
A study published on the preprint server MedRxiv on April 14 located seven studies of treatment with hydroxychloroquine (HCQ), four clinical and three observational. The abstract states:
The results of meta-analysis of clinical trials showed that there were no significant differences between patients who received the standard treatment with HCQ regimen and the patients that received the standard treatment without HCQ (RR: 1.44, 95% CI, 0.80-2.59).
…
This study indicated no clinical benefits regarding HCQ for treatment of COVID-19 patients. However, further large clinical trials should be taken into account in order to achieve more reliable findings.
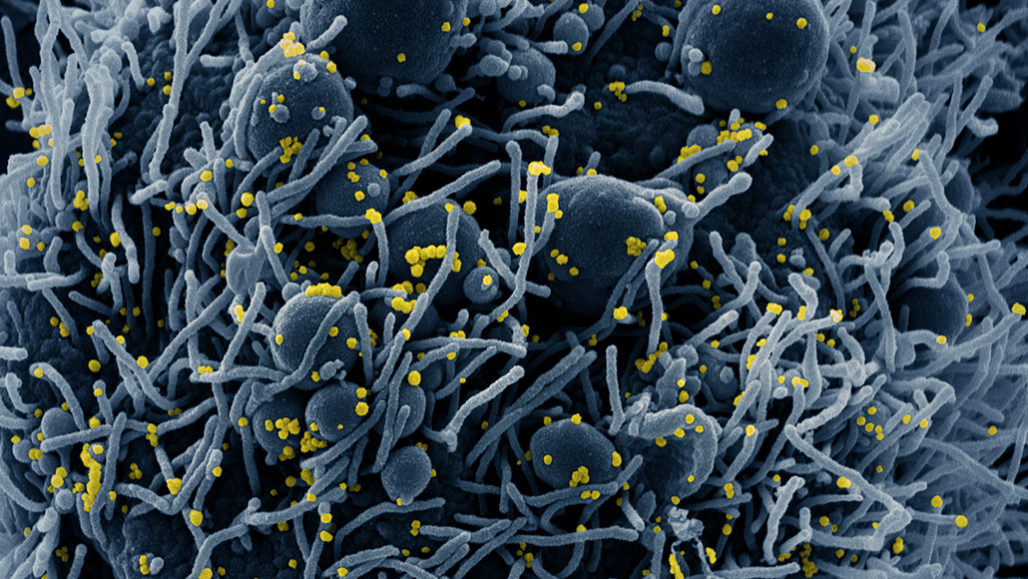
coronavirus electron micrograph from NIAID– CC license
A preprint article published in BioRxiv on April 16 (from China, supported by the Natural Science Foundation of China) identifies the tissues which express ACE2 on their cell surfaces and are thus susceptible to invasion by SARS-COV2. The researchers studied 31 different cell types and found many, previously unknown, that express ACE2. In order of sensitivity, they found that the lungs, nose, large and small intestines, the esophagus, fallopian tubes (parts of the uterus), and testis were identified as high-risk organs. The heart, kidneys, brain, and gall bladder were also found to express ACE2.
This study shows that large parts of the body are potentially infected by the virus. In particular, the nose and throat, the lungs, and the digestive system are exposed and must be readily infected. Spread of infection to the heart, brain, and gall bladder as well as the kidneys could occur in severe COVID-19.
There is evidence from other studies that an over-active immune system could be responsible for some of the manifestations in severe disease. Overproduction of cytokines (molecules that mediate inflammation) can cause extreme reactions in many infectious diseases. This appears to be a problem in patients who start to go downhill a week or so after infection.
The development of pneumonia and heart dysfunction (low blood pressure or heart failure) as well as mental or cognitive problems can be seen when the patient is suffering from severe infection. Even relatively mild infections are associated with confusion and hallucinations, especially at night.
These problems are happening to a small proportion of patients (perhaps 20% of apparent or symptomatic infections) but the most insidious aspect of this disease is the number of patients who have no symptoms at all, yet are secreting virus and thus contagious to others (this may happen in 30% or more of patients; the evaluation of sailors trapped on the Theodore Roosevelt found that 60% of virus-positive people were asymptomatic.)
As the virus spreads like a wildfire through the human population, we are discovering more about how it attacks the body. We are also learning more about how our bodies work.
The Chronicle of Higher Education published an article on April 17 reporting on the phenomenon of Twitter popularity as applied to Eric Feigl-Ding, an epidemiologist (his PhD was granted in 2007 in epidemiology and nutrition) with a voluntary one-year appointment as a visiting scientist in the nutrition department at Harvard. The specialty of nutrition in epidemiology is quite abstruse and there is a great deal of study in this area that tries to elucidate (make clear) the connections between what people eat and what illnesses they get or how long they live. None of it relates to infectious diseases, not directly– although a person’s susceptibility to infectious disease may depend on their nutritional status. For example, there is research suggesting that vitamin D deficiency increases a person’s risk for severe COVID-19.
His claim to fame is probably his tweet on January 25, stating that the R0 (the number of patients to whom each infected patient can pass on the infection) for SARS-COV-2 was 3.8. This number means that the virus will spread very rapidly if there is any contact between infected and susceptible people; not as fast as measles or chickenpox, but faster than we can handle without strict isolation, contact-tracing, and a vaccine.
Another epidemiologist, a professor of epidemiology at Harvard and director of the University Center for Communicable Disease Dynamics, described Feigl-Ding as a “charlatan exploiting a tenuous connection for self-promotion”. He pointed out that Feigl-Ding is not an infectious disease specialist, just a regular epidemiologist. Further, he stated that Feigl-Ding’s statements about the virus are “80% repeating conventional wisdom, 20% promoting wacko pseudoscience, and 100% derivative.” Finally, he said Feigl-Ding “gets something spectacularly wrong sufficiently often that you should find other parts of the firehose of info [information] to drink from.” I won’t give that man’s name because he doesn’t want to get backlash but really just wants to be left alone.
I can sympathize with this expert, who has real experience in “Communicable Disease Dynamics”, the science where the R0 is carefully studied (R0 isn’t applicable to nutrition in epidemiology). He doesn’t want people attacking him on Twitter and neither do I.
Eric Feigl-Ding, on the other hand, seems to court attention. He uses emojis, exclamation points, all-caps statements, and controversial claims liberally in his tweets. Calling him an unqualified publicity-seeker is at least half right– his qualifications do seem to be “tenuous”.
A source at Harvard “with knowledge of the situation” said that Feigl-Ding had “been asked many times to stop promoting himself as having specialized knowledge.” The article also says that “a University spokesman declined to comment on Feigl-Ding’s status.”
Here is a nearly perfect storm: someone who hungers for publicity (and Twitter followers), a global emergency, and at least a “tenuous” connection between that person’s specialized knowledge and the particulars of the emergency. This makes me sad.
Personally, I do not hunger for publicity, in fact I fear it (not that much, but enough). I nearly stopped posting altogether in my blog because of the impeachment circus. It was obvious to me that impeachment would not work, although I was disappointed by the spectacular failure of the Senate to even call witnesses like John Bolton. The disaster in the Senate and the inevitable but disgusting backlash that it inspired, the retribution/revenge that He-who-must-not-be-named exacted on his enemies and even those who did not sufficiently support him; all these things deeply depressed me.
Now, even the Steele dossier is being picked apart in the news media. As if it wasn’t made clear by Steele himself that the allegations made in his notes were not verified and may possibly have included Russian disinformation…
There are so many people with inadequate knowledge who claim to be experts, starting with the *president himself, who keeps saying that the test swabs (of which we are short) are made of cotton. To reiterate, cotton is unsuitable as a material for test swabs; synthetic materials like nylon or polyester are needed, and they have to be made in a certain way to maximize retrieval of virus from the samples. Even with the best swabs, the virus is only retrieved from about 75% of nasopharyngeal samples in known cases of infection. He-who-must-not-be-named has just said that he would invoke the Defense Production Act to mandate production of test swabs– although he didn’t give a timeline or say which company would receive the instructions. I do hope that they aren’t cotton swabs.
