
photo of a great-grandson by Mary Molina, copyright reserved
I have previously posted about the odd changes in emergency room visits that have occurred as a result of the pandemic. Normal emergency cases have suddenly disappeared; drops in heart attacks, strokes, appendicitis, car crashes, and other “normal” (expected) incidents have been observed. One thing that had not been remarked before is the disappearance of premature babies.
This article in the New York Times of July 19 details the drop in premature deliveries that has occurred in many hospitals since the pandemic began. The article begins with the observations of a doctor in Ireland.
According to the Times article, Dr. Roy Philip, a neonatologist at University Maternity Hospital Limerick in Ireland, noticed this when he first returned to his hospital in March at the onset of the lockdown. He found that demand for a milk replacement used by premature babies had vanished. When he ran the numbers, he found that premature births had dropped to a quarter of the average from previous years.
He published the results of his observations in MedRxiv as a “preprint” (not yet peer reviewed) report: compared to a historical rate of 8.18 (95% CI: 7.21, 9.29) per 1000 live births from January to April 2001 to 2019, 2.17 per 1000 live births was observed in January to April 2020. The rate ratio of 3.77 (95% CI: 1.21, 11.75), p = 0.022, represented a 73% reduction.
A Danish group reported similar results in MedRxiv on May 22. There, a registry of 31,180 live singleton infants born in Denmark between March 12, and April 14, from 2015 to 2020 was evaluated. “The extremely premature birth rate during the lockdown was significantly lower than the corresponding mean rate for the same dates in the previous years (odds ratio 0.09 [95 % CI 0.01 – 0.04], p < 0.001).” That is, a greater than 90% reduction in very premature births was seen.
Doctors in Rotterdam, Melbourne, and Alberta reported similar drops. The Times article continues, “In the United States, Dr. Stephen Patrick, a neonatologist at Vanderbilt Children’s Hospital in Nashville, estimated there were about 20 percent fewer NICU babies at his hospital than usual in March.”
The article states that not all hospitals have seen the same drop, although examples were not provided.
The causes for this dramatic drop during the last six months are unknown as yet. It is not even clear whether the drop is localized or general. Explanations could include reduction in air pollution, imposition of reduced activity outside the home, or many other changes unique to the lockdown. Whatever the reason, this is a fascinating finding and will certainly stimulate a lot of research.
Trends in premature birth in prior years:
In the US, premature deliveries have increased for the last four years in a row, according to the CDC. “White women had about a 9 percent risk of premature birth in 2018, while African-American women’s risk was 14 percent.” According to Statista, premature births in the US increased from 10.62% in 1990 to 12.8% in 2006, but then suddenly dropped to 10.4% in 2007 (perhaps a change in definition? It’s not clear.)
The overall birth rate dropped from 16.7 per 1,000 people in 1990 to 11.6 per 1,000 in 2018. That same year, there were 50 births per 1,000 women among White women and the same among Asian women. There were 54 births per 1,000 among Black women, 55 among Latino women, 59 among Native American women, and 67 among Pacific Islander or Hawaiian women.
According to CDC, premature births and low birth weight accounted for 17% of infant deaths in 2017.
Here is some general information about premature birth that you may find interesting:
Premature babies (“preemies”) are defined as those born before 37 weeks of gestation (normal is 40 weeks) and this occurs in about ten percent overall of US deliveries. Prematurity is more common in non-white mothers and those with fewer socioeconomic advantages. Prematurity is one of the leading causes of death for children born to non-white American mothers.
Preemies are faced with a variety of problems, starting with low birthweight (1500 grams or less; average babies weigh 2500 grams) and including underdeveloped lungs as well as heart defects and problems related to the reasons why they are born early. Premature infants are prone to vision and hearing problems, developmental delays, and cerebral palsy.
Premature delivery is most often heralded by amniotic sac breaking, leading to fluid leaking from the vagina. Uterine contractions may precede of follow the loss of fluid. Once the amniotic sac breaks, the baby must be delivered within 24 hours, or the risk of infection rises steeply.
Premature delivery is most often caused by infections including vaginitis (vaginal inflammation or infection) and systemic infections but often the underlying cause is unknown. Risk factors for prematurity include diabetes, high blood pressure, multiple pregnancy (twins or more), overweight or underweight, air pollution, tobacco use, alcohol and drug abuse, and psychological stress.
Treatment for premature birth:
Those at risk or having premature contractions can be treated with progesterone (one of two major female hormones, the other being estrogen.) Once delivery is inevitable, treatment with corticosteroids like dexamethasone and prednisone can improve outcomes, in part by stimulating maturation of the fetus’ lungs.
Nifedipine (normally used for blood pressure) and other drugs can reduce uterine contractions, delaying delivery. Once the baby is born, supportive treatment by warming, skin-to-skin contact with the mother, and oxygen supplementation aid survival. In extreme cases, it may be necessary to intubate the newborn and provide mechanical ventilation. Adding pulmonary surfactant (similar to detergent) to the oxygenated air greatly improves expansion of the lungs and therefore aids survival.
Complications of premature birth:
Premature birth is the most common cause of neonatal mortality; those born at 22 weeks’ gestation have about a 6% chance of survival, improving with each week after that, up to 72% at 25 weeks. Survival is often followed by numerous complications, from acute respiratory distress syndrome due to insufficient secretion of surfactant (called hyaline membrane disease) chronic lung disease (which used to be called bronchopulmonary dysplasia), blindness (sometimes caused by oxygen toxicity), bleeding into the brain (intraventricular hemorrhage, affecting 25% of those born before 32 weeks), to hypoxic-ischemic encephalopathy (brain damage caused by lack of oxygen.)
Other problems of prematurity include anemia, low blood platelets, high ammonia, low calcium, low thyroid hormones, and high bilirubin.
Normally, the fetus has a type of hemoglobin (Hgb) which has a greater affinity for oxygen than adult Hgb (fetal Hgb.) After birth, fetal Hgb is broken down and replaced by adult Hgb. Breakdown of fetal Hgb increases blood bilirubin levels, and this has to be metabolized in the liver. The newborn liver is not well equipped to do this work, and as a result, blood hemoglobin can rise rapidly. In addition, Rh-incompatibility can cause breakdown of red blood cells. A common and feared complication of elevated bilirubin (icterus) (signalled by yellow skin) can lead to brain damage (kernicterus) or death.
Icterus is common even in normal newborns and usually resolves spontaneously or through exposure to ultraviolet light (such as in sunlight) but if the level of bilirubin rises too high, it accumulates in the brain and kills nerve cells. Emergency treatment of high bilirubin is by exchange transfusion, in which the blood is replaced by equal amounts of normal blood.
If the ductus arteriosus (a bypass circuit in the heart which diverts blood from the lungs during growth in the womb) doesn’t close (known as patent ductus arteriosus or PDA) over time the pressure in the right side of the heart can increase and lead to right-sided heart failure. The earliest sign of PDA is low blood oxygen and shortness of breath. Normally the ductus arteriosus closes shortly after birth, but preemies often fail to close the ductus. and eventually show pulmonary hypertension (high pressure on the right side of the heart) and develop right heart failure.
Long term complications:
Nearly half of survivors born at 22-25 weeks of gestation have moderate to severe disabilities, including visual or hearing loss, cerebral palsy, and learning problems. Twelve percent have cerebral palsy and fifteen percent have hearing loss. Only 20 percent of these children are completely free of disabilities.
The 2007 Institute of Medicine report Preterm Birth found that the 550,000 premature babies born each year in the U.S. run up about $26 billion in annual costs, mostly related to care in neonatal intensive care units, but the real tab may top $50 billion.
The youngest known survivor of premature birth was born in San Antonio, Texas in 2014. She was born at 21 weeks 4 days and weighed 410 grams (14.4 ounces); she was attending preschool in 2018 and had a “slight speech delay” but was “otherwise normal.” The smallest known survivor was one of twins delivered by Caesarean section at 25 weeks gestation (due to the mother’s pre-eclampsia) in 2004 and weighed 261 grams (9.2 ounces) while her twin weighed 563 grams (1 lb 3.9 oz)… both twins had to have laser eye surgery to correct visual problems but were said to be otherwise healthy… (Wikipedia)
(Any otherwise unattributed information may be found in Wikipedia; I don’t make anything up.)
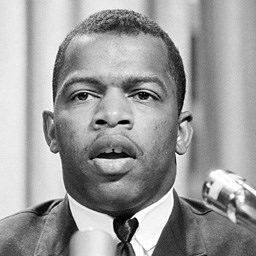
john lewis as a young man
John Lewis was born in 1940 in Troy, Alabama to a family described as sharecroppers; he was the third of ten children. He recalled later that by the time he was six, he had only seen two white people. His parents tried to teach him to live with things the way they were, but after he heard Martin Luther King Jr. on the radio when he was fifteen, he couldn’t accept it. He was drawn by Reverend King’s message of Christian nonviolence in search of human rights for black people, and he spent his life fighting nonviolently for his people.
According to this web page from history.com, on December 1, 1955, Rosa Parks (a member of NAACP since 1943) had been sitting in the first row of the seats reserved for “colored” people when the bus filled up and the bus driver demanded that she give up her seat so that a white man could sit. Three other black people in the same row stood up to accommodate the bus driver’s demand to turn the row into a whites-only row, but Ms. Parks refused. She later said that her feet weren’t tired after working all day as a seamstress at a department store, but she was “tired of giving in.”
She apparently already knew that the local chapter of the NAACP had been planning a bus boycott for months with Reverend King in the lead, but had been divided on its exact implementation. The boycott was in response to the law which had recently passed by the Montgomery City Council, requiring black riders to give up their seats to whites if the whites-only section of the bus was full. She was arrested by two officers who met the stopped bus, handcuffed, and taken to jail. She was released on bail later that night and scheduled for trial on December 5.
At trial, she was fined a total of $14– $10 plus court costs. The bus boycott, which began prematurely on December 5, lasted more than a year and deprived the bus line of the 70% of its riders who were not white. According to history.com, “On November 13, 1956, the U.S. Supreme Court struck down Alabama state and Montgomery city bus segregation laws as being in violation of the equal protection clause of the 14th Amendment to the U.S. Constitution.” On December 20, Reverend King called for an end to the boycott, and the next day, black riders including Rosa Parks returned. Most of the black ridership of the bus line had been walking to work for more than a year.
John Lewis attended the American Baptist Theological Seminary and Fisk University in Nashville, Tennessee, “historically black” educational institutions which granted him a bachelor’s degree in Religion and Philosophy. While still a student, he participated in attempts to desegregate lunch counters and attended workshops in nonviolence led by local religious leaders in the basement of the Clark Memorial United Methodist Church in Nashville. He was arrested many times for his non-violent demonstrations and attempts to desegregate downtown Nashville.
Student Non-violent Coordinating Committee
Mr. Lewis attended the conference that organized the Student Nonviolent Coordinating Committee (SNCC) in 1960 and became its chairman in 1963. SNCC grew out of the sit-in movement with the encouragement of the Southern Christian Leadership Conference (SCLC) as a commitment to “participatory democracy” instead of top-down leadership. SNCC developed a new strategy of not paying bail, in part to save money, but more to signal its opposition to the corrupt legal system which allowed people to be punished before (or without) conviction for any crime.
Mr. Lewis continued as chair of SNCC until 1966, when it was taken over by Stokely Carmichael, who emphasized “black power”. Thereafter, the SNCC’s influence waned and it was infiltrated by FBI agents.
One of SNCC’s first successes was the tactic of “kneel-ins” in which they knelt outside of white-only churches. In August 1960, the United Presbyterian Church’s 172nd General Assembly wrote to SNCC: “Laws and customs requiring racial discrimination are, in our judgement, such serious violations of the law of God as to justify peaceful and orderly disobedience or disregard of these laws.” (Wikipedia)
In 1961, Mr. Lewis became one of the thirteen original “Freedom Riders” who attempted to desegregate the interstate bus lines from Washington DC to New Orleans, Louisiana. Seven white people and six black people were the tip of the spear for groups like the Congress of Racial Equality (CORE) who wanted to help enforce the 1960 Supreme Court decision that declared segregation of interstate bus routes to be unconstitutional, invalidating multiple state laws. In response, the Federal Bureau of Investigation sent agents to tag along with the Freedom Riders. They did not intervene when the Riders were beaten and arrested on multiple occasions, but they did take notes.
President Kennedy called for a “cooling-off period” after the violent incidents and CORE abandoned the project. Mr. Lewis persisted, and was imprisoned in the Mississippi State Penitentiary for forty days. He was beaten in numerous bus stations, including Montgomery, Alabama. He said, “It was very violent. I thought I was going to die. I was left lying at the Greyhound bus station in Montgomery unconscious…”
The beatings will continue until morale improves…
Federal Legislation to achieve Civil Rights and Voting Rights
The federal government passed laws reinforcing the Supreme Court decisions and helping to implement the Fourteenth Amendment to the Constitution. President Kennedy proposed a law in June 1963 that was held up by a filibuster in the Senate. After Kennedy’s assassination, Lyndon Johnson took up the cause; after a 54-day filibuster, a law was passed in June 1964. It “outlaws discrimination based on race, color, religion, sex, or national origin. It prohibits unequal application of voter registration requirements, and racial segregation in schools, employment, and public accommodations.” (Wikipedia)
The law was supplemented by further legislation that asserted Congress’ authority to regulate interstate commerce, ” its duty to guarantee all citizens equal protection of the laws under the Fourteenth Amendment, and its duty to protect voting rights under the Fifteenth Amendment.” (Wikipedia) A year before the Civil Rights Act of 1964, an act called the Equal Pay Act of 1963 was passed which prohibited pay discrimination “based on sex.” Oddly, this act was added to the Civil Rights Act for controversial reasons– and was used by the Supreme Court in 2020 to bar discrimination against LGBTQ individuals. (See Wikipedia on the controversy under “Civil Rights Act of 1964– Women’s Rights“)
In 1964, the SNCC tried to organize a parallel Democratic Party primary in Mississippi which sent a delegation to the Democratic National Convention in August to challenge the all-white Mississippi delegation. The delegation was not allowed to be seated, despite the nationally televised testimony of an SNCC member who had been a sharecropper and had been brutalized attempting to register to vote. The black delegates were offered two “at-large” seats from which they could observe the convention but not vote. They turned them down and walked out.
Selma
Organized attempts to register black people to vote were violently resisted by the white establishment. Sit-ins at lunch counters in Selma, Alabama began after the bombing of a church in Montgomery on September 15, 1963 and were met with beatings and arrests. As chairman of the SNCC, John Lewis was a prominent member of the protests, and was among more than 300 people arrested in two weeks.
The Dallas County Voting League was organized to help blacks register to vote in Selma. Only two days a month were available for the public to come in to register at the courthouse. At one event, in October 1963, more than 300 blacks waited in line all day in an attempt to register; members of SNCC who tried to bring water to those waiting were arrested.
On July 6, 1964, four days after the Civil Rights Act was signed into law, John Lewis led 50 black people to the courthouse to register on one of the two allowed days that month; they were all arrested instead. Three days later, a judge issued an injunction forbidding any group of three or more people from assembling under the leadership of any civil rights organization.
The Selma Voting Rights Campaign began on January 2, 1965 (a day when the sheriff was out of town and couldn’t enforce the injunction) with a mass meeting led by Reverend King. On January 15, Reverend King called President Johnson, who agreed to start a big push to pass a strong voting rights act; Johnson also wanted to pass additional anti-poverty legislation. The local town police chief wanted to suppress violent anti-black activities (although he was still in favor of segregation) and he arrested a man who beat Reverend King. He also arrested George Lincoln Rockwell, the head of the American Nazi Party, who had come to town voicing violent threats against Reverend King.
The sheriff, however, controlled the block around the courthouse, and he continue to beat and arrest any blacks who tried to register. On January 25, 1965, a US District Court judge ordered that at least 100 people be allowed to wait in line to register at the courthouse; the sheriff arrested everyone over that limit. The demonstrations and violent arrests continued. On February 4, President Johnson made his first public statement in support of the blacks’ attempts to register to vote in Selma.
By the end of the month of February 1965, 300 black people were registered to vote in Selma (as opposed to 9500 white people.) During a demonstration in February in the nearby town of Marion, a protestor, Jimmie Lee Jackson, was shot by a state trooper and died eight days later; the trooper claimed that he had tried to grab his gun and there were no witnesses or video to contradict him.
Reverend King and the SCLC wanted to provoke a public outcry, but John Lewis and many in the SNCC were more concerned with trying to help people register to vote. Despite his reservations, Mr. Lewis agreed to lead a march with the Reverend Hosea Williams from Selma to Montgomery on March 7, 1965.
That march led to a confrontation on the Edmund Pettus Bridge in Selma. Between 500 and 600 marchers were stopped by a wall of state troopers and volunteers, some on horseback. They were brutally beaten and tear-gassed. Seventeen were hospitalized, and Mr. Lewis received a fractured skull (one of many beatings he endured at the hands of racists, for which he never fought back.)
The whole affair was televised, and national audiences were treated to views of peaceful black protesters being beaten unconscious by white thugs in uniform. President Johnson released a statement “deploring the brutality with which a number of Negro citizens of Alabama were treated.”
In 1965, the Voting Rights Act was passed after a national outcry over the vicious beating of black marchers on the Edmund Pettus Bridge in Selma, Alabama known as “Blood Sunday.” This law stopped “literacy tests”, poll taxes, and other racist impediments to voting registration that had prevailed across the southern United States.
This Act was eviscerated by the Supreme Court in 2013 when it declared a portion of it unconstitutional, making it impossible to enforce the requirement that certain states with a history of discrimination obtain prior approval before making changes to voting laws. See Wikipedia’s “Voting Rights Act of 1965” for details.
Outrage and Aftermath of Bloody Sunday
Bloody Sunday was only the most televised and best known of many beatings that black people have endured at the hands of racist thugs in uniform (and out.) Malcolm X planned to start fighting back, but he was assassinated. Many other nonviolent demonstrators were murdered. Black people are still being murdered at the hands of police, but not as many as in the past– a small improvement, to be sure.
However, as a result of national outrage over Bloody Sunday, the Civil Rights Act of 1965 made it possible for black people to register to vote and develop some political power. In places where they are a majority of the population, black representatives are carrying their voices in Congress as well as in local offices. In places where they are still a minority (which means most places) they can at least vote and demonstrate with some degree of safety.
Mr. Lewis was first elected to Congress in 1986, representing the 5th District, (which is 58% black and 99% urban), including the northern three-quarters of Atlanta, Georgia. He served 17 terms, dying in office yesterday. He was diagnosed with stage 4 pancreatic cancer in December 2019 and died on July 17, 2020. He is best known for his civil-rights activism and his adherence to non-violence, positions he shared with Reverend King. He was probably the last of the well-known civil rights activists from the sixties, and he was known as the “Conscience of the Congress.” He will be missed.
Obtaining the right to vote and the right to integrate public facilities is only the beginning. There are many things that are still separate and unequal. We can only hope that the end of the beatings will result in better morale.

Coronavirus studies by Engin Akyurt via pixabay.com
SARS-COV-2 enters human cells by attaching to a cell surface protein called the ACE2 receptor. The ACE2 receptor is found on the cell surfaces of epithelial (surface) cells in the lung, vascular endothelium (lining), and intestinal epithelial cells. It is also on vascular smooth muscle cells and the endothelium of the urinary tract (kidneys, bladder, and tubing). There is some ACE2 in the brain, but not as much as on the surface epithelium and vascular smooth muscle.
When it was first discovered in 2000, ACE2 was found at high levels in the kidneys(on the endothelial (lining) cells), heart (now known to be in heart muscle cells as well as blood vessels within the heart), and testis. Later, somewhat lower levels were found in the lung, vascular endothelium, vascular smooth muscle, and intestinal epithelium.
ACE2 functions in blood pressure control by relaxing smooth muscle lining the blood vessels. It does this by breaking down angiotensin II, which is a vasoconstrictor. Angiotensin II also has pro-inflammatory and pro-fibrotic effects. It is hydrolyzed (one amino acid is removed from its end) to angiotensin(1-7). This has the opposite effect to angiotensin II and “mediates vasodilatation, anti‐proliferation, and apoptosis…”
Normally, the body has a finely-tuned balance between higher and lower blood pressure. The kidneys balance retention of sodium and water with and excretion of sodium and water– this regulates total body blood volume and affects blood pressure. The inflammatory system balances between attacking foreign cells and proteins and accepting domestic cells and proteins. The body’s repair systems balance between killing off severely damaged cells (apoptosis), replacing them with scars (fibrosis), versus repairing mildly damaged cells and encouraging production of new cells. One of the balance-setting hormone systems is the renin-angiotensin complex.
There is some preliminary evidence that, when the virus invades an ACE2-bearing cell, it damages the ACE2 and leads to loss of function, causing a loss of the balance between angiotensin II and angiotensin(1-7). This seems to result in acute lung injury and respiratory distress syndrome. Invasion of the circulatory system may lead to increased blood pressure and an inflammatory cascade.
The most critical tissues directly invaded by SARS-COV-2 are lung epithelial cells, vascular endothelial (lining) cells, and intestinal epithelial cells. The virus gains entry to the body through the epithelium of the nose and through the lungs, but the nose is not severely affected. Instead, virus invasion of the deep lungs results in dry cough and shortness of breath. Most of the specific symptoms of infection relate to the lungs. Even in mild or asymptomatic cases, damage can be seen on lung computerized tomography (CT) and in pulmonary function tests.
The virus is responsible for diarrhea (sometimes watery) but not consistently– many patients do not experience intestinal symptoms. However, the virus readily invades the intestinal epithelium and virus RNA is consistently isolated from the stool. We do not know whether the virus can be transmitted by the fecal-oral route– all attention has been to the airways: droplet and aerosol infection.
Most cases also present with anosmia (loss of sense of smell) and/or ageusia or dysgeusia (loss or perversion of sense of taste) but this symptom is frequently overlooked. It is unclear whether this symptom is caused by damage to surface neurons in the nose and mouth, to epithelial cells, or even to deeper nerve cells in the brain.
/Update with data from article below:
Information From “New Understanding of the Damage of SARS-COV-2 Infection Outside the Respiratory System”
SARS-COV-2 invades the central nervous system through the olfactory nerves, and might also invade through nerves from the lungs. A patient with encephalitis was found to have the virus in his cerebrospinal fluid (CSF), and the authors of that case report worried that the virus might persist in the central nervous system even after apparent recovery. The presence of virus in CSF suggests that headache might be related to central nervous system infection; additional, more serious symptoms could be expected if encephalitis becomes established.
The “New Understanding” article discusses the possibility that gastrointestinal (GI) infection by consumption of an infected animal may have been the route of transmission for the initial jump from animals to humans. In cases where the GI tract is the infection route, we would expect diarrhea and other non-respiratory symptoms to predominate.
/End update
Fever, muscle aches and fatigue are prominent nonspecific symptoms that may be caused by the release of hormones that react to all viral infections rather than to specific invasion by the virus of tissues. The virus does not appear to invade immune cells in the blood or immune tissues like lymph nodes or bone marrow.
When the virus infection spreads beyond the lung epithelium, it attacks the vascular endothelium of the blood vessels and the smooth muscles of the capillaries. Here begin the more serious consequences of infection. Once the virus has invaded the blood vessels, we see the effects of the virus throughout the body, with small blood clots everywhere, reduced kidney function, high fever, delirium, reduced cardiac function, and so on. Oddly, virus RNA is usually not isolated from the blood; it is unclear what happens to the virus once it gets into the endothelium.
In autopsies, increased numbers of megakaryocytes (the cells that are parents to platelets) were found in the lungs and heart. Small and large blood clots rich in platelets (the cells that participate in blood clotting) were found throughout the body. Blood clots were found in the venous side of the heart as well as within the heart muscle. Prominent “acute tubular necrosis” (death of the kidney’s tubules) was found in most autopsies with tiny blood clots within the kidneys.
In all autopsied lungs, there was “diffuse alveolar damage” (breakdowns in the terminal sacs where oxygen is exchanged from the air to the blood) and the lungs were filled with fluid and pus. There were also signs of growth of new lung cells that were attempting to repair the acute lung damage.
The autopsy findings show that the lungs were the first site of infection, but damage to the kidneys and heart was prominent, and blood clots formed throughout the body.
This sketch shows the multisystemic nature of COVID-19 and how it relates to the ACE2 receptor and its normal function in the body.
Robert R. Redfield photo courtesy Wikipedia
Medscape reports on July 15 (see also ABC on July 14): In an online interview with the Journal of the American Medical Association on Tuesday, July 14, Robert R. Redfield, Centers for Disease Control (CDC) director, stated that the situation in the US (a currently out of control pandemic of COVID-19) could be brought under control within 4-8 weeks if “everyone wore a mask.” He also said, “I am glad to see the president and vice president wear a mask. Clearly, in their situation they could easily justify they don’t need to … but we need for them to set the example…”
That’s good, but consider the source. Dr. Redfield is another administration figure who got his post by being 1) highly religious; 2) a well-known figure among conservative activists. He has little experience running agencies and is over his head as director of CDC (although he apparently really wanted the job.) He is careful to avoid saying anything that might be seen as critical of his boss. He won’t be the source of scandal, but he won’t be a leader, either.
This article on CNN from June 4 (see this also for an even more jaundiced view) tells a lot more about who Dr. Redfield is and where his loyalties lie. He was described by former colleagues as a “bad leader” who put politics before science. He was also described as a loyalist to authority, making him perfect for this administration– which values loyalty above all else. Most important, he is close to conservative evangelists who think AIDS is a judgement from God.
Never mind that he worked on AIDS research for many years, first in the Army (he retired as a full colonel in 1996) and then in the private sector as a co-founder and former co-director of the Institute for Human Virology at the University of Maryland School of Medicine (which he started in 1996 with Robert Gallo, who is the current director.) Robert Gallo is famous (and notorious) in AIDS circles as the co-discoverer of HIV in 1984 (he admitted in 1991 that he had been sent a sample of HIV by the lab that first described it in 1983– and Gallo was left out of the Nobel Prize awarded in 2008 for the discovery of HIV.)
While he worked as a researcher on AIDS 1) Dr. Redfield promoted abstinence as a preventive measure for AIDS; 2) he derogated the importance of wearing a condom and “safe sex.” He clearly did this because of his religious views, in which abstinence holds a high place.
In 1992, Dr. Redfield deceptively edited early data about a vaccine for AIDS (based on the HIV gp160 protein) to make it look like it might be effective. This resulted in years of wasted studies trying to show this vaccine to be effective. It was not. That deception in the early stages of evaluation for the vaccine led to an Army investigation for Dr. Redfield. The investigation was dropped, but not before it left a bad taste in the mouths of many other AIDS researchers.
No other vaccine has emerged for AIDS, in part because the resources wasted on study of his vaccine left people thinking no vaccine could work. Drugs have come out that are highly effective for “pre-exposure prophylaxis.” The profits to be had from drugs to prevent AIDS far outstrip any potential profit from a vaccine.
A decision was made somewhere in the administration to bypass the CDC in reporting hospital data and to send the data directly and in secret to Health and Human Services “HealthProtect” where it can be manipulated before being selectively released to the public. This decision has only magnified the confusion around the data. Dr. Redfield was unable to prevent this knee-capping of the CDC and he said nothing about it in his interview yesterday– but today he says he supports it.
He did claim yesterday that the recent surge in virus infections down south was due to people from the Northeast vacationing down south over Memorial Day. This is to counter the widespread accusation that premature re-opening of southern states led to the increase in new cases– something his boss doesn’t want to hear.
No matter. We sincerely hope that he will lose his job in January. Otherwise, we will be in for more kakistocracy than this nation can handle.
Neurological and psychiatric complications of severe SARS infections: review and meta-analysis

EM of sars-cov-2 budding from apoptotic (dying) cells–NIAID
A review of psychiatric and neurological complications from SARS and MERS compared with COVID-19, published in Lancet Psychiatry May 18 (full text) assessed common symptoms associated with acute illness and after recovery by meta-analysis of multiple articles (65 articles and seven pre-prints were selected for quality and comprehensiveness) :
Neuropsychiatric symptoms associated with COVID-19
Acute neuropsychiatric symptoms of SARS and MERS (both diseases with much higher mortality rates but caused by closely related coronaviruses): confusion, impaired memory, insomnia, anxiety, and depressed mood. Post-illness (assuming the patient recovered from the acute illness): insomnia, anxiety, irritability, memory impairment, fatigue, depressed mood, and “traumatic memories” (similar to post-traumatic stress disorder.) Three-quarters of recovered patients had returned to work after three years of followup.
Neuropsychiatric symptoms associated with COVID-19: delirium (and confusion with agitation) occurred in two-thirds of patients admitted to intensive care. Altered consciousness on admission was seen in about 20% of patients who subsequently died. At discharge, a third of patients assessed had “dysexecutive syndrome” (difficulty in making decisions, apparently.)
Exact figures from the text:
Acute illness; “common symptoms among patients admitted to hospital for SARS or MERS included confusion (36 [27·9%; 95% CI 20·5–36·0] of 129 patients), depressed mood (42 [32·6%; 24·7–40·9] of 129), anxiety (46 [35·7%; 27·6–44·2] of 129), impaired memory (44 [34·1%; 26·2–42·5] of 129), and insomnia (54 [41·9%; 22·5–50·5] of 129). ”
Post-illness: “depressed mood (35 [10·5%; 95% CI 7·5–14·1] of 332 patients), insomnia (34 [12·1%; 8·6–16·3] of 280), anxiety (21 [12·3%; 7·7–17·7] of 171), irritability (28 [12·8%; 8·7–17·6] of 218), memory impairment (44 [18·9%; 14·1–24·2] of 233), fatigue (61 [19·3%; 15·1–23·9] of 316), and in one study traumatic memories (55 [30·4%; 23·9–37·3] of 181) and sleep disorder (14 [100·0%; 88·0–100·0] of 14)”
Meta-analysis: “point prevalence of post-traumatic stress disorder was 32·2% (95% CI 23·7–42·0; 121 of 402 cases from four studies), that of depression was 14·9% (12·1–18·2; 77 of 517 cases from five studies), and that of anxiety disorders was 14·8% (11·1–19·4; 42 of 284 cases from three studies). 446 (76·9%; 95% CI 68·1–84·6) of 580 patients from six studies had returned to work at a mean follow-up time of 35·3 months (SD 40·1)”
COVID-19: ” delirium (confusion in 26 [65%] of 40 intensive care unit patients and agitation in 40 [69%] of 58 intensive care unit patients in one study, and altered consciousness in 17 [21%] of 82 patients who subsequently died in another study). At discharge, 15 (33%) of 45 patients with COVID-19 who were assessed had a dysexecutive syndrome in one study. At the time of writing, there were two reports of hypoxic encephalopathy and one report of encephalitis.”
So these diseases shared similar mental symptoms during the acute illness and we would expect chronic symptoms after recovery to be similar as well. This is important, because about a third of patients demonstrated post-traumatic stress disorder after discharge. About 15% of these patients had anxiety or depression as well. Three quarters of them returned to work, but the study followed them for three years after discharge, so we would expect prolonged disability with COVID-19 as well.
Underlying Neurobiological Pathology in COVID-19
Another study published June 30 in the Journal of Alzheimer’s Disease described itself as reviewing the neurobiology of COVID-19 and postulated three distinct phases of infection. The article summarizes a number of published reports relating to neurological symptoms in acute infection. It says that there are a number of common symptoms that could represent direct invasion of nerve cells or a sign of the body’s reaction to the virus: “Anosmia, stroke, paralysis, cranial nerve deficits, encephalopathy, delirium, meningitis, and seizures are some of the neurological complications in patients with coronavirus disease-19” but it is not obvious what is the underlying cause (or causes) of these symptoms.
The three phases of infection hypothesized in the article are: first, direct invasion of cells lining the upper respiratory tract which express ACE-2 on their surfaces (ACE-2 is the protein to which the virus binds before it enters the cell.) Anosmia (loss of smell sensation) and dysgeusia or ageusia (perversion or loss of taste sensation) are, the article says, separate symptoms– and dysgeusia is actually more common than anosmia. Both symptoms, it says, are caused by direct virus invasion and damage to the epithelial cells of the nose, mouth, and throat.
By the same token, airway epithelial cells of the trachea and lungs are hosts to direct viral invasion and result in cough, dyspnea, and chest pain.
It is not known whether the virus can directly invade the brain through the cranial nerves and infect central structures responsible for processing of smell and taste signals, but it is presently considered unlikely.
The second source of neuropsychiatric symptoms is through blot clots in the arteries leading to the brain and in the veins draining blood therefrom. This is due to a hypercoagulable state (excessive blood clotting) which is brought on by pathologies associated with higher mortality: obesity, high blood pressure, and diabetes. In these conditions, levels of inflammation-related blood proteins like interleukins are already higher than normal and rapidly become even more elevated. These mechanisms are responsible for strokes, known as cerebrovascular accidents (CVAs.)
Some patients experience cerebral hemorrhages, which seems counterintuitive but appears to be related to vasoconstriction (closing of blood vessels by contraction of their intrinsic muscles.)
The third stage of brain injury in COVID-19 is also caused by excessive inflammation. In more severe cases, there is a “cytokine storm”, which involves the small blood vessels in the brain and results in leakage of blood proteins into the brain matter. Normally, the brain is protected by a membrane called the blood-brain barrier (BBB) which prevents all but a select few blood components from entering the brain. This barrier is tight enough to prevent many drugs that normally diffuse into tissues elsewhere in the body from entering brain tissue. When the endothelium (cells lining blood vessels) becomes inflamed, the BBB is breached and inflammatory molecules enter, damaging brain tissue.
The BBB breach causes symptoms of confusion, delirium, reduced level of consciousness (encephalopathy), seizures, coma, and death in extremis (at the end.) If a patient recovers from a partial BBB breach, he or she may be permanently disabled by memory loss and poor “executive function” (decision-making ability.) Depression, anxiety, and agitation are particularly common after recovery in these cases.
Some evidence suggests that SARS-COV-2 viral particles may, in some cases, directly enter the brain and infect neurons (some do have ACE-2 on their surfaces.) This may cause symptoms of meningitis and encephalitis: stiff neck, headache, and seizures. However, the virus has not been detected in cerebrovascular fluid as would be expected if there were direct viral invasion.
Cranial and peripheral nerves may be involved in COVID-19, similar to what was seen in SARS and MERS. There have been reported cases of Guillain-Barre syndrome (GBS) (flaccid paralysis with loss of reflexes and sensory loss or cranial neuropathy), caused by immune cross-reaction between nerves and the virus. These cases have responded to intravenous administration of immune globulin, typical of GBS. Therefore, these cases are not thought to be due to virus invasion of nerves but to immune reactions.
Heart and Skeletal Muscle Involvement in COVID-19
There is some evidence that invasion of cells with the virus leads to downregulation of ACE2 expression in the affected cells. This could lead to systemic effects of local invasion, by reducing the ACE-2 function, leading to hypertension, inflammation, and prothrombosis (increased blood clotting.)
Myocardial infarction in COVID-19 is thought to be due to the hypercoagulable state induced by severe inflammation. In addition, there is a suggestion that the nerves responsible for controlling the heart’s intrinsic rhythm may be involved by direct viral invasion. Early reports from Wuhan, China (also here) found frequent instances of arrhythmia and heart muscle weakness even in patients without myocardial infarction.
Viral invasion of heart cells would be described as myocarditis (heart muscle inflammation) as opposed to cardiomyopathy (weakness of the heart muscle caused by ischemia or other pathologies.) ACE-2 is expressed on the cell surface of many heart cells at high levels, including the heart’s smooth muscle (heart muscle, like other unconsciously controlled muscles, is smooth but skeletal muscle is striated.)
Skeletal muscles often show signs of involvement in COVID-19: the enzyme responsible for much of muscle’s activity, creatine phosphokinase (CPK), leaks out of damaged muscle cells and is found in elevated levels in the blood. However, direct injury of striated (skeletal) muscle appears unlikely because these muscle cells do not express high levels of ACE-2. High CPK appears to result from skeletal muscle injury by vasculitis (blood vessel inflammation) and other insults common to the intensive care unit (ICU.)
Skeletal muscles are weakened by the immobilization of serious illness and more so by the induced paralysis necessary to intubation and mechanical ventilation. This results in severe weakness after recovery; rehabilitation to regain strength is often prolonged.
Other Organs Likely to be Severely Affected by COVID-19
The cells that express the most ACE-2 on their surfaces are endothelium (the lining of blood vessels big and small), respiratory epithelium from the nose to the trachea, bronchi, and smaller tubes leading to the alveoli (tiny sacs in the lung where oxygen is absorbed into the blood), the lining of the digestive tract (mouth, throat, esophagus, small and large intestine– skipping the stomach itself which has a specialized lining that resists high levels of acid), the lining of the urinary tract (genitourinary endothelium– bladder, kidneys, and tubes in between), and smooth muscle cells (the heart and blood vessels, among others.) Damage from severe COVID-19 appears in all these organs, although it is most critical in the lungs (that fill with fluid, impairing oxygenation) and heart (where pump weakness and irregular beats lead to circulatory failure.) The brain clearly is involved in this cascade of disasters, whether directly or indirectly.
Patients Who Recover From COVID-19 Are Still Suffering Afterwards
I hope that this gives you a better idea of the spectrum of neurological and psychiatric symptoms associated with COVID-19. There is clearly a neurological basis for post-traumatic stress disorder, impaired memory, depression, and anxiety following the virus.
There are medical reasons why a previously highly organized and optimistic ER doctor would take her own life at 49 after appearing to recover from COVID-19 and returning to work. This case was reported on April 27. I won’t get into it in too much detail (here— NY Times, here–CNN, here–NBC, and here–NPR, are some news accounts), but there are reasons why someone with no predisposing psychological problems would kill herself– it’s the pernicious effects of the virus combined with the unreasonable and unrealistic demands that were placed upon her as an emergency room physician and director.

credit squeeze– photo by steve buissinne courtesy of pixabay.com
The Washington Post has an article on July 14 reporting that big banks have seen significant drops in their profits and are increasing their credit reserves in anticipation of multiple defaults on their loans. They apparently expect a prolonged recession as a result of the pandemic. Prolonged recession will turn into a depression.
The pandemic prompted people to stop going to public events and going out to eat or for entertainment. State governments ordered shutdowns for restaurants, bars, concerts, movie theaters, barber shops, hair stylists, tattoo parlors, bookstores, and many other establishments– anything nonessential. Only supermarkets, pharmacies, gas stations, and other “essential” businesses (like gun stores) were allowed to remain open.
Economic activity dropped dramatically in March. Advertising revenue for newspapers plummeted as businesses stopped placing ads for public events. Millions of people were laid off. In the United States, Statista showed a drop in employment from 128 million in March to 114 million in April. So many people tried to file for unemployment that state agencies charged with registering them were unable to keep up. As a result of the backlog, millions of people were unable to file. According to Statista, “As of June 2020, there were 120.17 million full-time employees in the United States. This is a significant decrease from June 2019, when there were 131.54 million…”
These numbers (a drop of more than 10 million employees) are almost certainly an underestimate. Unemployed people were unable to pay their rent or keep up the payments on their cars or credit cards. As a result, the banks are experiencing a sudden loss of revenue from people defaulting on their loans. Now the banks are anticipating that this drop will continue to affect their revenues for some time to come.
A sudden, severe recession, with people unable to feed themselves or pay rent, is going on right now. A slight improvement in employment for June will soon be followed by further job losses and a prolonged recession. Starvation and homelessness are on the rise. Congress responded to this crisis with legislation in March and April but nothing since then. Another Congressional stimulus is expected towards the end of July, but it will not be enough to relieve the suffering of millions in this country.
Here is a comment to the Washington Post article:
Finally getting through to business executives and Fed officials that no matter how high the stock market gets boosted by liquidity among the wealthy, people who are afraid they will die if they leave their home will not be spending much money even if they kept their jobs. And millions of unemployed will be spending MUCH less once the extra $600 / week federal unemployment top-up stops in a couple of weeks. So 70% of the economy is going down the toilet. Yet the stock market is flying high. Don’t you love trickle up economics!
This comment points out that the stock market, after dropping almost a third at the start of the crisis, has recovered most of its value despite the worsening infection numbers and death count. Even people who still have their jobs are afraid to go out. They are not spending online either because they are afraid that their jobs are at risk even though they are still employed. Lower consumer spending will perpetuate the recession and the job losses.
The stock market represents the fortunes of the upper half of society, which will do well despite the pandemic and will become increasingly divorced from the fortunes of the lower half, which will sink into depression.
This pandemic is even worse than the one a hundred years ago. During the 1918-1920 influenza pandemic, 675,000 Americans were killed and an estimated 50 million people worldwide died (cdc historical page.) We hope that not that many people will die this time, but it is still early. What makes this pandemic worse than that one already is the severe economic impact. Back then, the economy was mostly made up of manufacturing enterprises; now, the economy is mostly consumer-oriented. Manufacturing continued then, but now, consumer spending has cratered.
What makes things worse this time is that concerted action by the federal government could prevent the spread of the virus. If the feds organized testing, contact tracing, and isolation, there would not be so much confusion, shortages, and political infighting. Instead, the federal government’s executive branch leadership has consistently denied or downplayed the virus’ impact and refused to get behind public health measures. Lower level attempts by the CDC and others to offer guidelines and provide information has been undermined by ignorant behavior at the highest levels.
Nothing has been done at the federal level to organize supplies needed for testing or personal protective equipment. Shortages of everything are as bad as they were at the beginning. The leadership has denied that these shortages even exist.
On top of the pandemic, police brutality and murder has been captured on cell phone videos starting on May 25, stimulating an outraged response by minority people, their representatives, and the persuadable public at large. Police brutality (especially towards minorities) has existed since time immemorial, but it has never been seen so widely as now. Public protests about police brutality have been met with more brutality instead of understanding. The problem has reached a tipping point. Broad social change is resulting. Again, the federal government executive branch leadership has not responded in a constructive fashion.
The result of the presidential failure to respond to the pandemic and public realization that police brutality is ongoing is extreme social polarization. A majority of the public is aware that the pandemic is spreading out of control and that the police are as brutal as ever, but a large minority is in denial and is violently resisting calls for change. Society has long been deeply polarized, but matters are worse now than they have ever been.
The nation will soon come forth to vote in presidential elections which will probably see the present administration fall. That will not be the end of the battle. Just as before the Civil War of 1861, the election will result in crystallizing society into two opposing groups. Violent conflict will follow.

photo by nastya_gepp courtesy of pixabya.com– chosen because it’s not her.
The administration’s pressure to open all primary and secondary schools this fall and cut off international students from colleges that don’t re-open has two purposes. First, to score political points by making it look as if the Democrats are trying to keep schools closed for nefarious purposes. Second, to cause chaos and disruptions in public schools that will make charter schools and home schools more attractive by comparison. Part of the underlying motivation is to advance the administration’s goal from its opening days of spending billions of dollars to subsidize charter schools and vouchers for home-schooling parents. Betsy DeVos is part of the plan.
Betsy DeVos sat for a TV interview the other day. She chose this moment (Sunday, July 12) to make herself available because she has a message for the public: “open schools this fall, with in-person attendance for everyone, or we will cut off your funding.” (That’s a paraphrase, because what she actually said was obviously a talking point that had been drilled into her by an aide.) What she really said:
American investment in education is a promise to students and their families. If schools aren’t going to reopen and not fulfill that promise, they shouldn’t get the funds, and give it to the families to decide to go to a school that is going to meet that promise.
She said this repeatedly, in response to multiple questions, without any variations or any attempt to provide substantive answers to the big questions: 1) how can you insist on sending children back to school in the middle of a pandemic without a clear plan for preventing the spread of infection? 2) what makes you think you can unilaterally cut off funding to schools that don’t comply with your demands?
She had no answers for these vexing questions. There is no federal plan to guide schools in preventing spread of infections, from child to child and from child to teacher (or to janitors, for that matter.) There is no funding for the extra expenses that an infection-prevention plan would entail. There is no legal way the executive branch can cut off funding to the schools; most of the money for schools comes from local and state sources and is inaccessible to federal executive action. What money does come from federal sources is mostly earmarked for special programs for disabled and disadvantaged children, and could not be cut off simply by executive decrees.
This is a mischaracterization of why we are taxed to support public education. We don’t “invest” in education; we pay taxes to support teachers and schools, who in turn teach classes and provide activities that help children and teenagers learn things that we think are important to their careers and civic responsibilities. An investment implies a contract with an expected rate of return, in money. The returns we expect from spending money on schooling are not monetary– they are primarily an intangible benefit to society.
We could monetize the returns by calculating how much money people would make if they didn’t go to school versus how much they will make after graduating– and then divide out how much more they will pay in taxes for their better-paying jobs– but that would miss out on the intangible benefits. How do we calculate the monetary value of an educated populace to our society when they use their knowledge to elect good leaders, to comply with just laws, to live longer, more satisfying, and healthier lives because they understand the benefits of good diet, good hygiene, a balanced life, exercise?
In fact, the public educational system serves multiple purposes. First, for modern families, it is a place to put children while their parents are working– to prevent them from being left alone during the day (in the past, children not in school were employed on the family farm.) Second, it is a way to teach children things (so many different things.) Third, it is a place for children to play and socialize, and learn how to get along with others
Betsy DeVos was appointed to her post because she is rich, conservative, an evangelical Christian, and good-looking. She has no relevant experience in the field of education. Her education ended with a baccalaureate degree majoring in business economics (she might as well have majored in art or literature if she cared about education.) She is the daughter of a billionaire who made his money in the auto parts supply business in Detroit. Her husband is a former CEO of Amway (a “multilevel marketing organization”, or more bluntly, a successful pyramid scheme.)
She is politically active, starting with her work for the presidential campaign of Gerald Ford while she was in college. She was chair of the Michigan Republican Party. Her brother is Erik Prince, who founded Blackwater, a supplier of mercenaries to the US military (which became notorious after some of its men massacred 17 civilians at a highway intersection in Baghdad in 2007.)
She came to the attention of the current president because of her family’s monetary support for the Republican Party. She openly admitted in a Roll Call op-ed in 1997 that her family was the largest single contributor to the Republican Party in Michigan, and that she was essentially buying influence. She did not publicly support the president until after the election; the only public statement I could find was a comment from March 2016 in which she described him as an “interloper” who “does not represent the Republican Party.” Her family did, however, spend $2.7 million on Republican candidates and PACs in the 2016 election cycle.
Just how much influence became immediately apparent when the incumbent president announced a couple of weeks after the election that she would be nominated to the Secretary of Education post. This is despite the fact that she did not publicly support him before the election– afterwards, she did make some positive statements. She was one of the first Cabinet members for the new administration to pass through the Senate. She was confirmed by the Senate on a vote of 51-50 in which the Vice President had to come in to cast a tie-breaking vote; she did not even receive all the Republican Senators’ floor votes for confirmation.
Two Republican Senators, Susan Collins and Lisa Murkowski, voted against her confirmation, despite having voted in committee to move her nomination to the floor. Clearly their voting positions were intended to send a message that they were providing the minimum of support required of them. Their weak support may have been influenced by the Democrats’ vociferous opposition. This was the first time a nominee to a Cabinet position was confirmed by a tie-breaking vote from the Vice President in a very, very long time.
Despite scraping through the Senate, Ms. DeVos has remained on the Cabinet ever since– quite an accomplishment for the present administration and making her one of the longest-serving Cabinet members, along with Ben Carson and Mrs. Mitch McConnell. They have all retained their positions by keeping their heads down, avoiding scandalous spending, and not granting interviews.
Ms. DeVos has a very clear agenda: she wants to defund public education in the United States and substitute charter schools and home schools. What money she would support spending would be in the form of payments to families with children so they could be being home-schooled, preferably in a religious curriculum. She has been consistent in pushing this agenda throughout her career, including… her early leadership of the “Great Lakes Education Project.” This “project” pushed the establishment of “charter schools”, which are publicly supported but privately run educational institutions.
Michigan, and Detroit in particular, became the center of the US charter school movement partly as a result of her backing. The movement has led to hollowing out of public schools, especially in underserved areas like central cities. Detroit is a particularly egregious example of the effects of this movement. As its population dropped and became more minority-dominated, funding became ever weaker. The charter school movement allowed private companies to run schools with support from public funds, further draining the public schools of public support. This New York Times article from 2016 describes the disastrous results.
Ms. DeVos wants to substitute home schooling and a few charter schools for our public school system. She wants to reduce funding for schools overall and substitute a tax break for families that home school their children. This is primarily an excuse for families to religiously educate their children at home rather than pay for them to be educated in public schools alongside minority children. Public schools, in the view of her supporters, are godless communist indoctrination systems. Charter schools, as private institutions from their point of view, would have more leeway and motivation for religious instruction.
All of her claims that poor children are left behind by public schools are so much gaslighting. Poor families can’t afford to home school their children. They need the public schools to keep watch on and feed their children during the day so that both parents (when there are two parents) can work, and make enough money to support them. Grandparents in poor families are not strong enough to care for children at home during the day, if they have not already died from the novel coronavirus.
Betsy DeVos has been a very effective advocate for quietly defunding public schools under the banner of charter schools. She has been destroying them from the inside, just as most of the current president’s Cabinet members have tried to destroy the Environmental Protection Agency, the Consumer Financial Protection Bureau, the Centers for Disease Control, and other executive branch agencies. The damage that this president has done to our federal government is immense and will take years to undo. All the more reason for us to vote in eight years of Democratic administrations, with a House and Senate to match.
Coronavirus studies by Engin Akyurt via pixabay.com
This report on Vox.com was published on July 12: “My patient caught Covid-19 twice. So long to herd immunity hopes.” In the report, a doctor in Washington DC describes one of his patients a 50 year old man, who had COVID-19 twice, the first time as a mild illness, the second time more severe. He had a mild cough and sore throat the first time, three months ago. The second time, a couple of weeks ago, he had high fever, dyspnea (shortness of breath), and hypoxia (low oxygen levels in the blood.)
In between, he felt well for at least six weeks, and had two negative PCR (polymerase chain reaction, an antigen test for acute infection) tests. He was exposed to another member of his family (“a young adult”) with the virus. He was not able to get an antibody test after the first infection, so we don’t know if he had developed antibodies– which makes a big difference.
Other reports of similar cases have occurred, including this one from central New Jersey. Two patients were reported by a doctor there, including one who had developed antibodies and donated plasma to treat other patients infected by SARS-COV-2. Apparently both patients were from the same family. The doctor who made this report also posted a video to Facebook, which I did not consult as I am averse to that particular medium.
We don’t know what these cases of reinfection mean or how common they are. We don’t know how many people are susceptible to getting sick again. We do know that laboratory tests of rhesus monkeys showed immunity after repeat challenge with known dosages of the same virus. The likelihood is that most people will be immune but some will not. It is also possible that there is more than one strain circulating, although the known mutation that caused increased efficiency of infection (without showing worse infections) apparently had the exact same antigenic characteristics.
After all that has been done to research this virus, there is still much that we don’t know. The number of cases is rapidly increasing, so rarer complications and more unusual cases are surfacing. What these things mean will not be revealed for some time.
As to Facebook: it may be a useful tool for making connections with people and exchanging information, but it is also a dangerous time-sucker. I am averse to being used as a commodity. I have avoided that platform for the last year. Other media are available for communicating information and I don’t think I am missing anything by not going there.

photo by Manfred Antranias Zimmer courtesy of pixabay.com
(The following descriptions should be seen as a simplification based on the Wikipedia texts that describe the concepts of the two religions, the Vedas, and other specific pages. I tried to make sense out of them but only succeeded partially. Some of what I’ve written is correct, some is oversimplified; I’ve tried to avoid obvious errors but if Wikipedia is mistaken, then I’ve just repeated the mistakes. If you know differently, please tell me.)
Buddhism and Hinduism share their origins in the Vedic literature of northern India (circa 1500-500 BCE.) Brahmanism can be thought of as the precursor to Hinduism; its rituals were recorded in the Vedas. Hinduism asserts the authority of the Vedic scriptures but Buddhism criticizes them. Brahmanism was preceded by Vedism– the religion described in the earliest Vedas.
Vedism was the religion of the Indo-Aryans who migrated into the Indus River basin circa 1500 BCE. It is described in the Vedic literature, including the early Upanishads. In Vedism, there was an afterlife but no reincarnation. Ancestor worship was prominent, with rites like offerings of food; this declined but did not completely disappear in Hinduism. Vedism is described in Wikipedia as a complex animistic religion, with pantheism. Vedic rituals that survived into Brahmanism and Hinduism include (among many others): fire rituals, horse sacrifice, cow sacrifice, royal consecration, and cremation. Human sacrifice is alluded to in the Vedas, but whether it existed in pre-Vedic times is highly controversial.
Vedism included the gods Indra, Agni, and Soma among many others. Hinduism began with the change in emphasis from these gods to others: Vishnu and Shiva especially. The hymns of Vedism described in the Vedas were given a different interpretation by Brahmanism and Hinduism.
In this period, the concept of rebirth developed and the afterlife was changed; ancestor worship was de-emphasized. Jainism, Hinduism, and Buddhism all adopted the idea of rebirth. The concept of rebirth includes the doctrine of samsara, an eternal cycle. In this cycle, a person is reborn after death, but not necessarily into another human body. As a result of karma, you can be elevated or degraded. A particularly bad person may be reborn as a cockroach. A good person will be reborn into a higher caste and eventually into a Bodhisattva or enlightened being.
The religions share basic concepts that include dharma and karma. Briefly, dharma is the “law” or prescriptive doctrine which everyone is obligated to obey. Karma is a kind of causality, the effect of obeying or disobeying dharma. Karma is not necessarily an immediate result of one’s behavior. The consequences may not play out in someone’s present life, but be carried over into one’s next life.
Brahmanism probably began with the “monist” (unifying) doctrine of Brahman, or the universal soul. This universal soul was postulated to be at the center of all living things and also the unifying principle of the cosmos. Brahmanism also brought together people into a system of castes.
Basic caste (varna) theory holds that each person is born into a certain category, of which there are four: brahmin (scholars and priests), kshatriya (warriors, kings, and princes), vaishyas (farmers, merchants, and artisans), and shudras (workmen and service providers.) Not mentioned in the original caste theory are untouchables, who are outside the caste system. The theory of caste, although based on ancient Vedic scripture, was not practically applied in India.
Instead, a system called “jati” or birth groups was applied in practice. There were many categories of jati, each applying to a hereditary group of specific occupations. The varna categories were actually applied by the British when they took over control of India and Pakistan in the eighteenth century and thereafter. This made the caste system more rigid, which is ironic considering the criticism of its static nature applied by British sources.
What distinguishes Buddhism from Hinduism (and Brahmanism) is the Buddhist emphasis on fluidity of one’s merit, regardless of caste. To a Buddhist, what matters is one’s behavior, not one’s caste, in accumulation of merit. Ordination as a priest is available to people of all castes in Buddhism, whereas a Hindu priest had to be a brahmin. Buddhists did not deny castes, but felt that a person’s caste was a reflection of their behavior in a past life rather than an “accident of birth.”
This brings us to the concept of liberation, called “moksha” or “nirvana” depending on the religion. The ultimate goal of existence is liberation from the cycle of samsara or rebirth. To reach this stage, one must first live in harmony with dharma or the rules. Then one must become enlightened. This is achieved through jhana, which is usually done in meditation but can occur spontaneously. The Buddha reached jhana momentarily during his childhood in a particularly auspicious time of perfect calm.
To Buddhists, it is necessary to have the correct perceptions– the permanent transcendence of the belief in the separate existence of the self is integral to the enlightenment of an arhat or arahant (enlightened one.) The most important difference between the two religions is their disagreement over the existence of a permanent, separate self or atman– Buddhists say there is no cosmic self. Instead, there is a state of change or impermanence called anicca and a void called shunyata. There is no true self and no universal self– there is only non-self, anatman or anatta.
All sentient beings are capable of enlightenment, eventually. Sentience is a quality of being that can include plants as well as animals, although it is more remote for more vegetable beings (even non-organic items like rocks can sometimes be described as sentient.) During one’s experience of samsara (rebirth), one cycles through many sentient objects or bodies, possibly including rocks.
Wikipedia says that sentience is characterized by specific qualities: “Sentient beings are composed of the five aggregates, or skandhas: matter, sensation, perception, mental formations and consciousness.” Plants are capable of sensation (light and touch, for example), but perceptions may not be present. Whether perception, mental formations, and consciousness are characteristics that plants share is questionable.
This is important because both Buddhism and Hinduism share the dharma of ahimsa: nonviolence towards sentient beings. The concept of ahimsa starts in the Rig Veda and is extended throughout the Vedas. A hymn to Indra in the Rig Veda (the earliest Veda) mentions satya (truthfulness) and ahimsa. The concept gradually developed during the Vedic period, from a mention of meat consumption and animal sacrifice as being undesirable to, eventually, elimination of sacrifices and promotion of vegetarianism.
The Jain sect of Hinduism, already well-developed in the early Vedic period, emphasized ahimsa as its first principle and included vegetarianism from the beginning. Even in consuming vegetable foods, roots were frowned upon because pulling them up kills the plant and involves violence against soil organisms. Consuming yeast-made bread, fermented foods, beer, and wine are now forbidden to Jains because the micro-organisms in such foods are killed (before the invention of the microscope, no-one knew that yeasts were living organisms or that bacteria existed.) Previously, intoxicating beverages were proscribed for Jains only because they impaired thinking rationally about non-harm.
Ahimsa imposes restrictions on warfare and self-defense but allows violence to preserve the lives of potential victims. Cruelty to one’s opponents and harming noncombatants, however, is considered always wrong. Negotiation in an attempt to prevent war is strongly encouraged. The doctrine of ahimsa is most famous in the work and thought of the Mahatma, Mohandas Gandhi. Wikipedia says: “In Gandhi’s thought, Ahimsa precludes not only the act of inflicting a physical injury, but also mental states like evil thoughts and hatred, unkind behavior such as harsh words, dishonesty and lying, all of which he saw as manifestations of violence incompatible with Ahimsa.”
Both Buddhists and Hindus agree on ahimsa as an essential part of dharma. They both practice meditation, although in different ways. They also agree on the use of mantras, which are symbolic phrases or poems that help in attaining concentration when one meditates (and for other purposes.) The word “yoga” is shared between the two religions but seems to mean different things– in Hinduism, it means the binding of one’s soul to the universal soul through physical means. In Buddhism, it appears to mean any spiritual practice, including tantras.
I have to stop here. No more work today. I’ve been reading too much scientific stuff which makes it all too clear that our country has a major crisis that is not being addressed by the current government. The only clarity I’ve gotten is in the importance of ahimsa and the difference between brahman (universal soul) and anicca (impermanence). I’m going to go back to the beginning and start again tomorrow. Let me know if you can articulate where I’m mistaken– please.

S Hermann and F Richter photo via pixabay.com
Someone we know, who was a friend, died from COVID-19 today after being in the hospital for two weeks. We’re not surprised (but we still don’t think he should have died, and in a just world– not this planet– he wouldn’t have died…) We will miss him, but his wife will miss him more.
